https://mobeensyedmd.substack.com/p/increased-emergency-cardiovascular?s=r"
Increased emergency cardiovascular events associated with vaccine rollout in Israel among 16-39-year-olds, study finds.Association does not prove causation but further study is urgently needed.
KoolBeens Cafe
May 6
A retrospective population-based
study that analyzed call data from Israel’s National Emergency Medical Services (IEMS) found a more than 25% increase in calls for both
cardiac arrest and
acute coronary syndrome among 16-39 year-olds during the first 5 months of 2021, as compared to the years 2019-2020.
1 While cardiac conditions are caused by COVID-19 and are also reported as side effects of the vaccines, the peer-reviewed study published in
Scientific Reports found that the emergency calls were “significantly associated” with the rates of 1st and 2nd vaccine doses administered to this age group, but not with COVID-19 infection rates. All of the vaccines administered in Israel were manufactured by Pfizer.
The authors say the findings “underscore the already established causal relationship between vaccines and myocarditis, a frequent cause of unexpected cardiac arrest in young individuals.”
Messenger RNA vaccines manufactured by Moderna (mRNA-1273) and Pfizer (BNT162b2) have been associated with an increased risk of myocarditis, especially in male adolescents and young adults. According to the United States
Centre for Disease Control—drawing on self-reported data from the
Vaccine Adverse Event Reporting System (VAERS)—myocarditis has been reported typically after the second dose and within a week of vaccination.
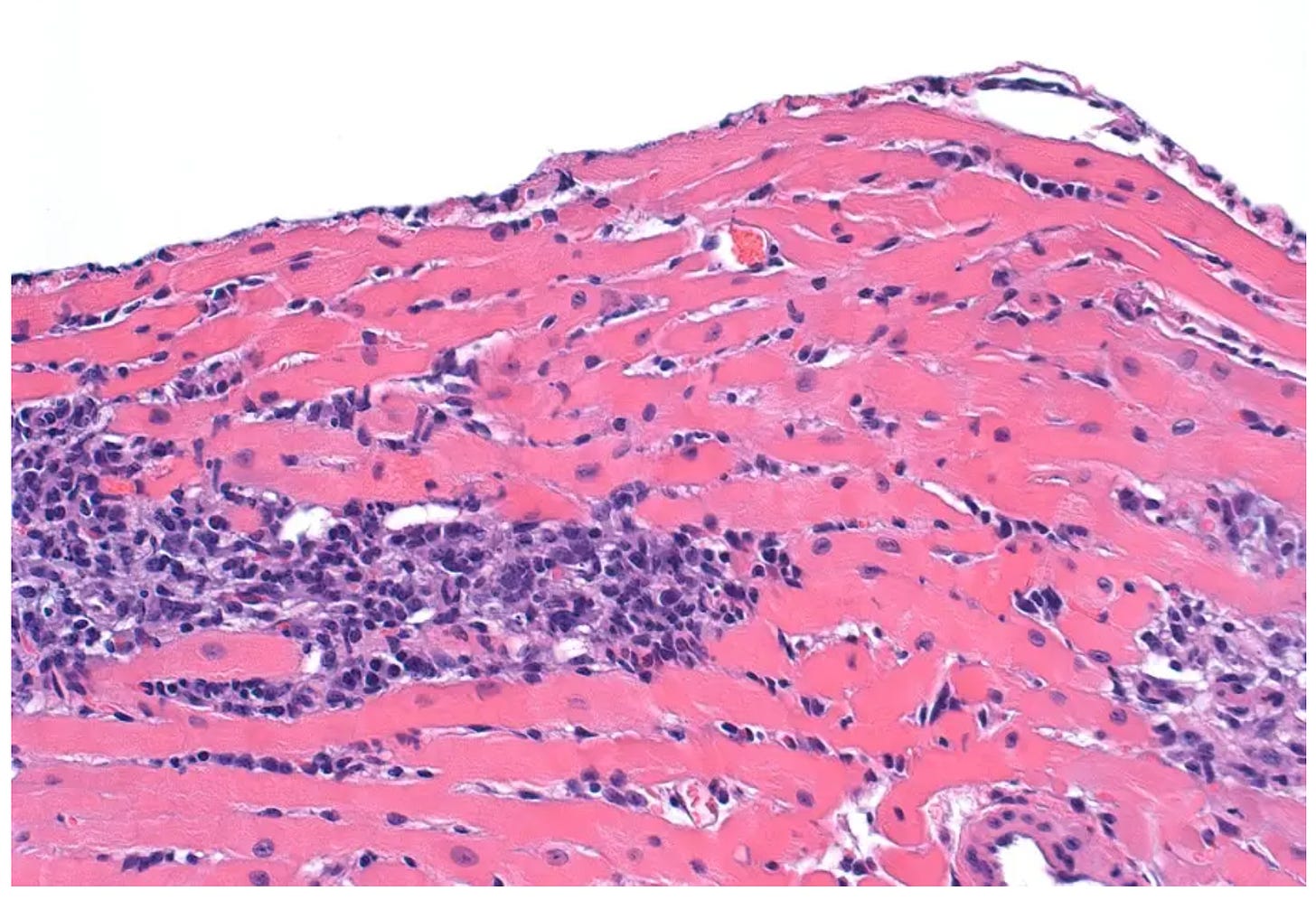
Myocarditis in a mouse heart. Cardiac inflammation stains purple.
Myocarditis Foundation.
Myocarditis causes inflammation of the heart muscle, which enlarges and weakens the organ, and creates scar tissue forcing it to work harder to circulate blood and oxygen throughout the body. Myopericarditis is inflammation of both the heart muscle and the layer (pericardium) surrounding the heart. According to the
Myocarditis Foundation, the inflammation can be in response to a viral infection, or some other trigger including autoimmune diseases, such as rheumatoid arthritis or lupus.
Combining emergency call data with pandemic waves and vaccination ratesThe study combines IEMS call volume data for cardiac arrest (CA) and for acute coronary syndrome (ACS) with data on COVID-19 infection rates and vaccination rates over a span of two and half years, divided into three time periods: a 14-month “normal period” beginning in January 2019, prior to the pandemic; a ten-month “pandemic period” starting in March 2020, which includes two infection waves; and a “pandemic and vaccination period” from January to June 2021, which includes a third wave as well as Israel’s vaccination rollout for those aged 16 and older.
Here are some of the main observations (see Figures below for more detail):
Cardiac arrest calls (red line) appear to be decoupled from pandemic infection waves (grey line).
The increase in cardiac arrest calls (red line) appears to be associated with the vaccination rollout (purple and blue lines for 1st and 2nd dose respectively) and not with third wave (grey line).
The increase in cardiac arrest calls (red line) appears to be highly associated with the 2nd dose of the Pfizer vaccine (blue line).
The increase in cardiac arrest calls (red line) after April 2021 is associated with the single vaccine doses administered to individuals who were previously infected and recovered from COVID-19 (green line).
While the association between CA calls and the 1st and 2nd doses of vaccine seems to be a convincing one, the same cannot be said for the association between the single vaccine dose (green line) and the second spike in cardiac arrest calls (Figure 2). In this case, there seems to be a disconnect rather than an association.
To view the Figures relating to acute coronary syndrome (ACS)—which showed a similar association with Israel’s vaccination rollout— please
go here.
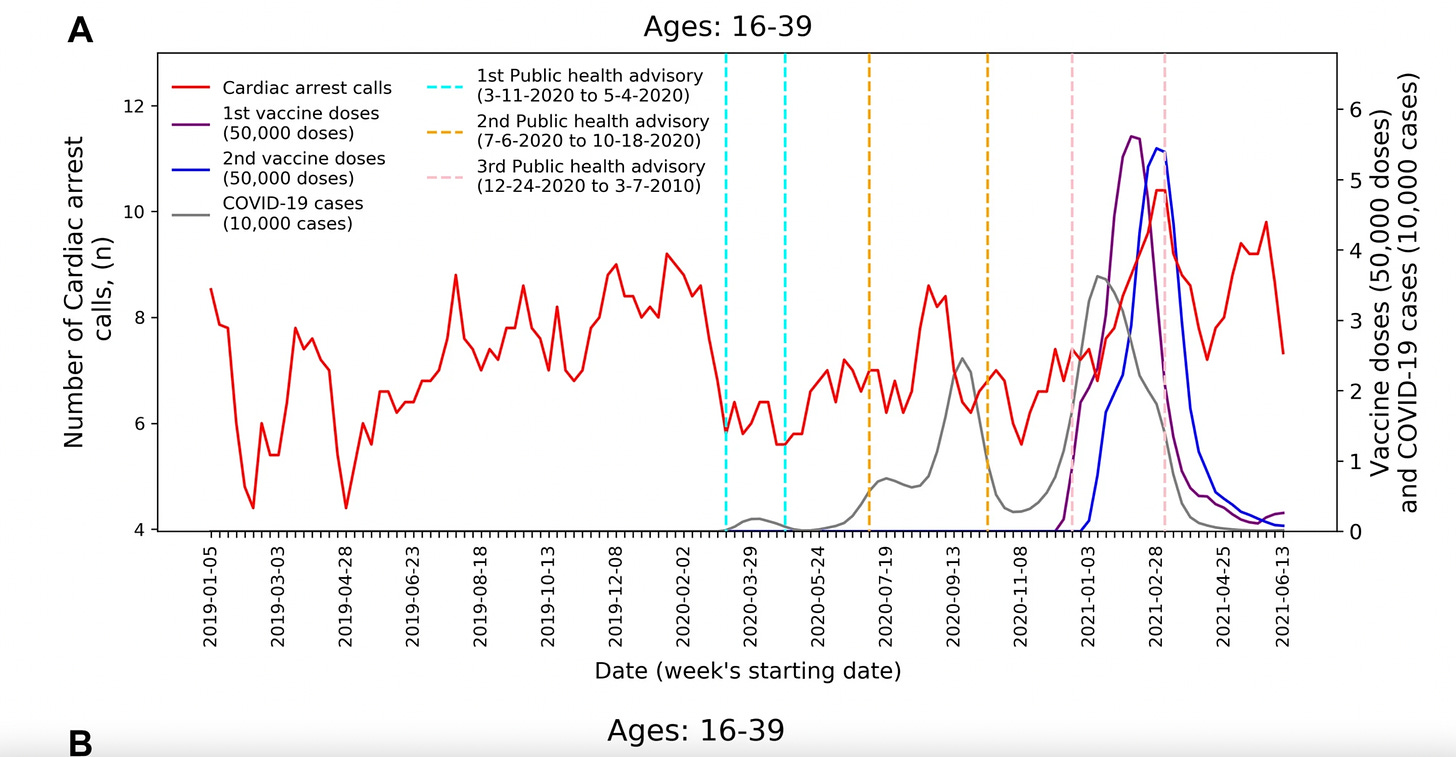 Figure 1: Number of cardiac arrest calls (red line) from January 2019 to June 2021. Screen shot taken from IEMS call study (2022).
Figure 1: Number of cardiac arrest calls (red line) from January 2019 to June 2021. Screen shot taken from IEMS call study (2022). 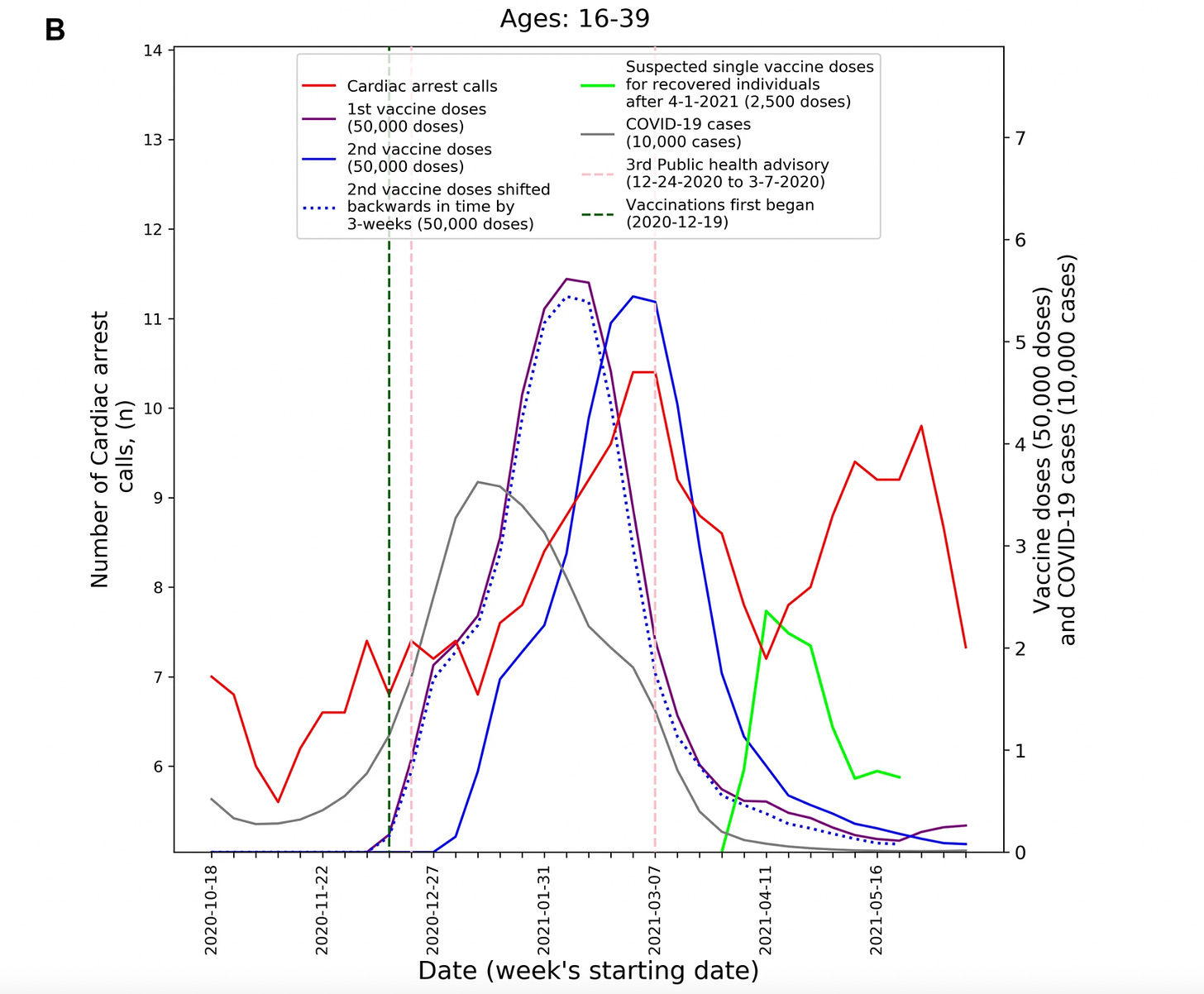 Figure 2: Number of cardiac arrest calls (red line) during the “pandemic and vaccination” period only. Screen shot taken from IEMS call study (2022). Cardiac tissue changes can persist for months
Figure 2: Number of cardiac arrest calls (red line) during the “pandemic and vaccination” period only. Screen shot taken from IEMS call study (2022). Cardiac tissue changes can persist for monthsWhen a group of patients aged 12-17 years, who presented in hospital with mRNA vaccine-related myopericarditis returned for follow-up 3-6 months later, the majority continued to have “abnormal” heart MRI findings. This is
according to a paper published in the
Journal of Pediatrics, which was discussed
in detail here. The authors of the study—most from the Department of Pediatrics at Seattle Children’s Hospital—say that while abnormalities persisted, function had improved. They say the findings raise concerns for “potential longer-term effects” and plan to repeat the cardiac MRI on these patients at the 1-year postvaccine mark to re-assess.
The key point here is that when myopericarditis occurs, whether it’s a result of COVID-19 or the vaccine, there can be remnant damage to the heart and the signs of fibrosis and scarring can persist in a patient for a long time.
Who’s at higher risk, males or females?The IEMS call data study also stated that while vaccine-induced myocarditis has been predominantly reported in males, the data indicate that the relative increases of CA and ACS events was larger in females. “This may suggest the potential underdiagnosis or under-self-reporting of myocarditis in females,” they write.
This observation seems to be supported by the findings of a
population-based study published late last year in the
British Medical Journal that found that Moderna’s vaccine was associated with a significantly increased risk of myocarditis or myopericarditis in the Danish population, compared with the unvaccinated, “primarily driven by an increased risk among individuals aged 12-39,” while Pfizer’s vaccine was only associated with a significantly increased risk among women.
At the same time, however, a
population-based study out of Israel published in the
New England Journal of Medicine (NEJM) found that young male recipients of the Pfizer vaccine had the highest risk of myocarditis: a rate of approximately 1 per 26,000 males compared to 1 per 218,000 females after the 2nd vaccine dose. It also noted that the “incidence of myocarditis declined as the number of newly vaccinated persons decreased over time,” saying this was “suggestive of a possible causal relationship,” that may be related to the mRNA sequence that codes for the spike protein, or to the immune response that follows vaccination.
These varied findings about myocarditis risk suggest an urgent need for further investigation.
Share KoolBeensCafeCritics of the Israel emergency call data study misrepresent it Almost immediately after the IEMS call data study was published, an organization called
Voices for Vaccines, a program of
The Task Force for Global Health, tweeted the following:
_____________________________
What they found was there was a significant increase in these events for young people (16-39) right around the time when Israel was vaccinating its population, but no overall association with COVID-19 infection rates. They suggest the vaccine may be the cause…Let’s start with the obvious: correlation isn’t causation. The actual science of the paper is simply showing a correlation, without controlling for much.2_____________________________
However, as previously stated, the authors were clear that the study “[did] not establish any causal relationships” but did nevertheless “raise concerns regarding vaccine-induced undetected severe cardiovascular side-effects and underscore the already established causal relationship between vaccines and myocarditis.”
The authors of the IEMS call analysis reference a number of studies (other than their own) that do establish a “probable causal relationship” between the messenger RNA vaccines and the adenovirus vaccine with myocarditis “primarily in children, young and middle-age adults.” These studies can be found
here,
here,
here,
here and
here.
Contrary to what Voices of Vaccines asserts, the authors take great pains not to attribute causality by explaining that cardiac events are also prevalent among COVID-19 patients, and that since vaccine rollouts took place during community spread of the virus, identifying the driver of increased incidence “could be challenging.” They also say the increases in calls could be tied to “underlying causal mechanisms indirectly related to COVID-19,” such as patients “delaying seeking emergent care because of fear of the pandemic and lockdowns.”
The authors openly acknowledge the “main limitation” of the study:
_______________________
[It] relies on aggregated data that do not include specific information regarding the affected patients, including hospital outcomes, underlying comorbidities as well as vaccination and COVID-19 positive status. Such related data are critical to determine the exact nature of the observed increase in CA and ACS calls in young people, and what the underlying causal factors are.
_______________________
They also point to a key “policy implication”—one that is hardly controversial: EMS data should be incorporated into the current vaccine safety surveillance systems, along with self-reported data, to help identify public health trends, and to better understand “the risk-benefits of the vaccine” to “prevent potentially avoidable patient harm.”
In sum, the study used emergency service calls—a unique data source—which should be incorporated into our own vaccine safety surveillance systems, and the study findings warrant further investigation.
Watch Dr. Mobeen Syed’s summary video about the IEMS call
study here.
1 There was a statistically significant 25.7% increase in calls for cardiac arrest (CA) and a 26% increase in calls related to acute coronary syndrome (ACS).
2
The Task Force for Global Health is an NGO based in Atlanta, Georgia, and is
funded by corporations including pharmaceutical companies (18%), government, including the US CDC (58%), as well a number of foundations (19%).For more information about the Task Force and Voice for Vaccines, please take a look at this
2017 article by Peter Doshi, Associate Editor with the British Medical Journal. As the article is dated, funding amounts need updating.
KoolBeensCafe is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber."
Read the whole story on
CoolBeens Cafe.


