Presentation and discussion by medical and legal professionals:
Shedding Is Real: FLCCC Weekly Update (Nov. 01, 2023) (34 minute video with discussion by clinicians following)
https://rumble.com/v3tb41v-shedding-is-real-flccc-weekly-update-nov.-01-2023.htmlPlease read the article at the source as I can't capture it all here. I enlarge font and bold parts I find are most outrageous.
https://pierrekorymedicalmusings.com/p/shedding-of-covid-mrna-vaccine-componentsSkip the preface and go directly to article at first bold and enlarged font.
Very few would not remember the immediate complaints by UNvaxxed women at the time of vaccine rollout, regarding the radical changes in their
menstrual cycles and bleeding, that could pretty much only be explained by vaccine component shedding by their vaccinated husband and/or others around them - since that was the only change - while the rest of us were instructed by Big Pharma's-captured lying mainstream media, that we were simply not supposed to believe what those women observed, about their own bodies through their own eyes.
Even today there is no shortage of denials from Big Pharma's propagandists and fellow profiteers in government, media, academia, medical journals, self-proclaimed "fact checkers", etc. etc. with the same line.
So it's up to each individual to investigate and think for themselves and consider the
evidence on all of the issues - some subjects of which are highlighted in this forum section - compared to other "news" sources and decide for oneself. If you log in I can help you find or explore a subject you're interested in. Also, the forum search function works very well to explore information that has been collected in this forum for over 3 years.
As has been suggested since even before vaxx rollout, the board members and employees of the corporations responsible for this global mass homicide, along with their facilitators in government and censors in digital and print media, need to make a decision as to whether they would prefer to come forward and as witnesses or wait until they are compelled to come forward as defendants. Stock market players are already sniffing out the securities fraud angle which will bring down Pharma's house of cards. Early birds will establish little need for those that come forward late.
On to the thread subject by imminently qualified ICU pulmonologist Dr. Pierre Kory:
https://twitter.com/PierreKory(Folks with an interest in free speech should establish an account at X (formerly Twitter).)
https://pierrekorymedicalmusings.com/p/shedding-of-covid-mrna-vaccine-components“Shedding” of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated - Part 1
It's happening. The manufacturers and regulators knew it was a risk, yet, like numerous aspects of the Covid vaccine mRNA technology, did not test for excretion potential of spike proteins or LNP's.
Pierre Kory, MD, MPA
Nov 1, 2023Awareness of the Federal Regulators and Vaccine ManufacturersThe data showing the toxicity and lethality of the vaccines started within weeks of the roll-out with hundreds of thousands of adverse events and hundreds of deaths reported to VAERS in January of 2021, far
exceeding previous stopping points of any new medical product or vaccine.
Although ignored (to this day), anyone paying unbiased attention could see a further mountain of evidence develop, including
a skyrocketing number of newspaper and television reports of healthy athletes and young people arresting and dying while doing normal everyday activities or sports (countered by corporate/government controlled media with a plethora of fact checking articles using cherry picked data to inform the world that what they are seeing is not factually true).
Then
life insurance industry data emerged showing historically unprecedented rises in death claims being paid out amongst the healthiest sectors of society
temporally associated with the proliferation of Covid mRNA vaccine mandates within schools, corporations, universities, health care institutions, federal contractors etc. Most telling of the deathly impact of mandates was the fact that the
largest increases among the sudden, rapid rises in excess deaths occurred among employed white collar workers.
The reality is that these data are still ignored by media and public health agencies across the world. Even more worrying are the more recent reports finding universal contamination of every studied vaccine vial with large magnitude, excess levels of DNA fragments and DNA plasmids. Then the discovery that the DNA plasmids used in the manufacturing process contained genetic sequences that both promote DNA integration into the human genome as well as promote the development of cancer.
It truly is unimaginable that we now must consider the risks (and reality) of “shedding” of the vaccine products from the vaccinated to the unvaccinated. This now has implications for nearly every human being walking the earth, vaccinated or unvaccinated (including me).This series will explore the regulatory, scientific, epidemiological, and clinical data indicating that shedding is occurring. The health of who knows how many is now being threatened, with the extent of the risks likely both highly variable and difficult to predict, both in the short term and long term. That is unless we start to seriously study the phenomenon further. So, let’s review what is known.
Within 3 months of the rollout of the global Covid mRNA vaccination campaign, I was consulted by two different unvaccinated women in their late 30’s and early 40’s respectively, who reported that they were suffering acute menstrual abnormalities in the days following close exposure to a recently vaccinated practitioner (one visited a massage therapist and another an acupuncturist). Both had a history of highly regular, uncomplicated menstrual cycles over decades.
Since that time, at least twenty other unvaccinated and vaccinated people, both men and women, have reported to me compelling histories of typical post-mRNA vaccine adverse effects subsequent to close exposure to vaccinated family members, contacts, or friends.
Further, my partner Scott Marsland at our
Leading Edge Clinic, who also specializes in treating Long Covid/Long Vax syndromes, has a growing series of detailed case histories of similar “shedding” events occurring. I will revisit this in a later post in this series, but I will briefly say here that our clinical observations conclude that symptomatic shedding events do occur. However, we have little idea of exactly how common it is occurring among the general population.
This is further complicated by the fact that even if it were occurring frequently, the vast majority of people suddenly developing typical vaccine side effects symptoms after exposure to a vaccinated person would never think to relate it to exposure to shed vaccine products. It is my belief that very few people in the general public are aware of the possibility it could occur. You know, because the regulators have assured the country that mRNA technology is “safe and effective.”
However, my general sense is that it occurs largely in people who have increased physiologic sensitivity to environmental exposures, toxins, or pharmaceuticals and that it is generally transmitted by someone recently vaccinated or someone who is producing a lot of spike protein. Note that is my “general sense.” More studies are required to fully understand both the frequency of and physiologic impacts from such events.
My ignorance as to the frequency of symptomatic shedding events is due to the fact that the concept of transmitting spike proteins (or lipid nanoparticles) from a Covid mRNA vaccinated person to another is one of the least studied and published-on aspect of the mRNA vaccine technology.
What is so shocking about that lack of research (actually nothing is shocking anymore) is that shedding has major global implications. Apparently it is not just me who thinks this because, as an expert on several aspects of Covid, I have been lecturing across the U.S, Europe, and South America in conferences, Parliamentary hearings, or invited lectures. Questions about shedding appear everywhere (in the dozens of Q & A’s that I have participated in, it is nearly always the first question. It is also a very common topic in the chat of our
FLCCC weekly webinar.
Know that in this tonight’s FLCCC webinar (
Wednesday 7p.m EST), I will be presenting a 15-20 minute overview of this series along with my private practice partner Scott Marsland. We expect to be deluged with questions after.
As a physician committed to education, I (finally) decided to respond to the void of information around shedding with this series of deeply researched posts. If you appreciate the effort, please consider supporting
my commitment to continuing this Substack with a paid subscription (I have been debating whether to give it up due to too many competing demands of my time - help me make that decision :).
Go to the link to this article to subscribe:
https://pierrekorymedicalmusings.com/p/shedding-of-covid-mrna-vaccine-componentsAnyway, I believe that by the end of this series on the science, epidemiology, and clinical observations of shedding, you will be convinced that it can and does occur.
What IS The Definition Of Shedding In Regards To The Covid mRNA Vaccines?From our Federal government, in this
FDA document, the term “shedding” is defined as:
“
The release of viral or bacterial gene therapy products from the patient by any or all of the following routes: feces (feces); secretions (urine, saliva, nasopharyngeal fluids, etc.); or through the skin (pustules, lesions, sores).”
They forgot to mention “exhaled breath.” More on that later. The “products” they refer to that can be transmitted from a Covid vaccinated person to another include not only the genetically programmed spike protein product, but also the lipid nanoparticle (LNP) containing the mRNA that is in the injections as well as naked mRNA that can be released from the LNP. Even more worrying is the recent shocking discovery that every single Moderna and Pfizer vaccine vial is contaminated with high levels of DNA plasmids potentially capable of integrating into the human genome. Contemplating that last one is disturbing, the implications of which we will not know for some time.Why Would The Modified mRNA Vaccine Technology Lead To The Possibility of Shedding?First off, let’s be clear that the Covid mRNA and DNA vaccines are
gene therapy medicinal products (GMTPs or GTP’s) as stated in the FDA’s
2015 document on Gene Product Shedding Studies.
“
Gene therapy products are all products that mediate their effects by transcription and/or translation of transferred genetic material and/or by integrating into the host genome and that are administered as nucleic acids, viruses, or genetically engineered microorganisms.Also note that in this European Medicines Agency
(EMA) document, the mRNA vaccines also meet their definition of gene therapy medicinal products (GMTP’s).
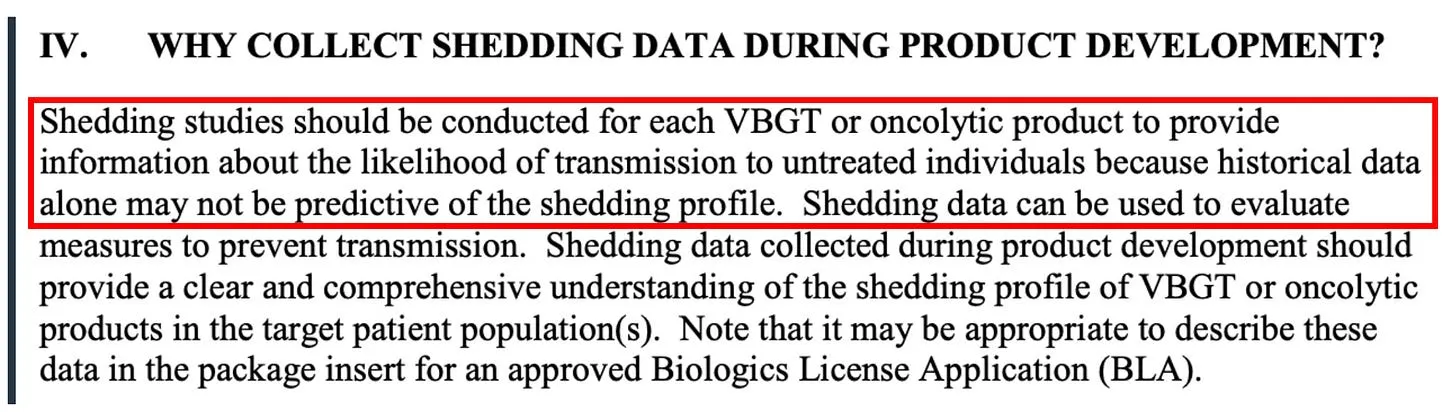
Ok, now that we know what a gene therapy product is and that the Covid mRNA injection is actually a form of gene therapy (marketed to the public as a “vaccine”), what does that have to do with “shedding?” Again from the FDA document regarding the evaluation of the safety of gene therapy products, they emphasize the importance of studying shedding:
Shedding is distinct from biodistribution because the latter describes how a product is spread within the patient’s body from the site of administration while the former describes how it is excreted or released from the patient’s body. Shedding raises the possibility of transmission of virus or bacteria based gene therapy products (VBGT) from treated to untreated individuals (e.g., close contacts and health care professionals).
This guidance represents FDA’s current thinking on how and when shedding data should be collected for VBGT and oncolytic products during preclinical and clinical development and how shedding data can be used to assess the potential for transmission to untreated individuals.So, with these findings in mind, it may be no wonder why the FDA insists on shedding studies:
Further on in the document, the FDA again emphasizes the importance of shedding studies:
Note that the FDA emphasizes the importance of doing
human shedding studies and not just relying on animal studies:
To inform the design of human shedding studies, shedding data may be collected in animals following administration of the VBGT or oncolytic product. These data can help estimate the likelihood and potential shedding profile in humans, particularly when there is concern about transmission to untreated individuals. However, such data cannot substitute for human shedding studies for several reasons.
But again, no studies testing whether excretion of mRNA-containing LNPs, modified spike-encoding mRNA, or spike produced by vaccinated people have been done. Well, I shouldn’t say none, because in this paper the author cites a Pfizer document obtained by FOIA which apparently revealed that shedding was studied in the urine and feces of intra-muscular injected rats. Unfortunately, that document is no longer at the website referenced.
To summarize from the above, the FDA’s position is that:
the mRNA vaccines are gene therapy products
Gene therapy products require shedding studies in both animals and humans
Gene therapy product shedding raises the possibility of transmission from treated to untreated individuals
Note that much of the rest of this series of posts on shedding is guided by a masterful comprehensive review of the topic of gene therapy product shedding by independent researcher (by definition) Helene Banoun in Infectious Diseases Research. Hers is one of the only papers I could find that attempted to meticulously explore what is known about shedding of the mRNA gene therapy vaccines.
As already stated, an important point Banoun makes is:
There was no regulation of mRNA clinical trials prior to RNA vaccines, yet there is strict regulation of gene therapy products. It is difficult to justify that mRNA vaccines are not considered in the same way as gene therapies regarding this regulation; indeed the only difference is that they are (historically) supposed to protect against a disease and not cure it. Gene therapies are intended for a small number of people in poor health, whereas vaccines are used on a large scale on healthy people: it would therefore be wise to apply stricter rules to them.She further points out another omission of the regulatory process:
Any experiment involving the deliberate transfer of a nucleic acid to a human must be preceded by Institutional Biosafety Committee approval (document on the regulatory standards is here), but approval was not given because of the emergency clearance given to mRNA vaccines.
Therefore, according to both the American and European agencies, mRNA vaccines are gene therapy products and should have been subjected to excretion studies of all secreted fluids (urine, exhaled droplets, saliva, sputum, nasopharyngeal fluids, semen, breast milk, feces, and sweat). Again, these studies were not done for mRNA vaccines nor for the DNA adenovirus vaccine (J&J).So, where are the clinical human shedding studies? Well, I just learned of one that is about to be published (next ten days?) where the research team exposed a population of unvaccinated women to vaccinated individuals and their assessment outcome was the development of menstrual abnormalities. I know the results but want to respect the research teams right to present their original work. They have promised to share their manuscript with me and Paul Marik as soon as the peer-review and acceptance process is complete. I have no idea what journal they submitted to but I can be highly confident it is not the New England Journal of Medicine.
The entire reason why I did a “deep dive” into shedding science is because shedding was not studied when it absolutely should have been and I believe with near certainty that it occurs. Note my use of “near certain” is only to seem objective but it really is too late for that - both my partner Scott and I have diagnosed and successfully treated a number of shedding “victims.”
The lack of shedding studies prior to the mRNA rollout was, in my opinion, an insanely reckless and irresponsible omission (or willfully criminal, take your pick). As an
evolving expert in the evaluation and treatment of Covid mRNA vaccine injury syndromes, I and others have identified the spike protein as the main component responsible for not only the
pathogenicity of Covid but also of the vaccines, with
this review paper proposing a new field named “spikeopathy” (study of the disease processes triggered by the spike protein).
If vaccine transcribed spike protein can be transmitted in sufficient quantity from vaccinated folks to unvaccinated ones, it stands to reason that adverse effects of the vaccine can develop in some unvaccinated people who came into contact (or close proximity) with vaccinated people. How did they get away with not studying this possibility?
An easy answer is they were doing science at “warp speed.” The more uncomfortable answer is that the “vaccines”, although meeting the definition of a gene therapy product, were actually not even legally considered a medical product at all and thus did not require a diverse range of safety studies (like on genotoxicity, reproductive risks, excretion potential etc). What? Why? How?
The reality is that the Covid vaccines, as a result of successive federal legislative actions which evolved over decades, was legally categorized as a “countermeasure” under a “public health emergency.” Such “countermeasures” require no specific regulatory approval process prior to dissemination. All a countermeasure needs is the recommendation of the Secretary of Health and Human Services that “it may be effective.” This is the conclusion derived from the legal investigatory work of various independent and legal experts and researchers like
Catherine Watts, Todd Callender, and Sasha Latypova. If interested in learning more, I would watch this
lecture by Sasha Latypova (scroll down the page to find her lecture). As they have uncovered, “countermeasures” (even gene therapy ones) do not legally require studies of excretion potential, bio-distribution, pharmacokinetics, genotoxicity, insertional mutagenesis etc.
They don’t even require FDA regulated clinical trials of efficacy or safety.
So why did Pfizer and Moderna even do the efficacy trials? Latypova maintains that they did this not only to satisfy the public’s confidence to increase vaccine uptake, but also to “fool” the public into thinking these vaccines were medical products subject to standard (albeit accelerated) pharmaceutical product regulatory processes.
This obscured the reality that they were instead classified as military “countermeasures” against a perceived (if not actual) bioweapon. To wit, the COO of Operation Warp Speed was a General from the Department of Defense (DOD) and the vaccine manufacturers were under contract with the DOD to produce the countermeasure, sometimes referred to as a “demonstration (demo)” and/or a “prototype” in numerous legal documents they uncovered. Anyway, as a result of this lack of a legal requirement to fully study these products in a public health emergency, the list and types of studies that should have been conducted (but were not) is long. Researchers and clinicians have been screaming about this since they were rolled out. These cries were met with a deafening silence by governmental health agencies across the world.
I know, it is a lot to take in.
But the latest “word on the street” is that the finance and insurance industries may finally be waking up to this fraud and its devastating impacts on U.S disability and death rates. Knowledge of these society-wide impacts largely results from the work of two different research teams led by former Blackrock portfolio manager Ed Dowd and insurance industry consultant
Josh Stirling).
This article describes the reasons why Pfizer and Moderna stock are crashing of late. Put more succinctly, from what I hear it is due to the hedge fund guys shorting their stock.
I believe Pfizer is in even deeper trouble now that this “forensic” paper just got published finding that they hid vaccine trial deaths which obscured a 3.7 fold increased risk of cardiac death in the vaccinated arm of their trial.https://www.nakedcapitalism.com/2022/02/bankruptcy-for-moderna-definitely-pfizer.html  https://pdfs.semanticscholar.org/1d79/a14307e35646b8fd9209fc8a17e12d2d6ca9.pdf
https://pdfs.semanticscholar.org/1d79/a14307e35646b8fd9209fc8a17e12d2d6ca9.pdfLinks to all the other (already active) posts in this series is after the subscribe button below.
P.S. I just want to say thanks to all my subscribers, especially the paid ones! Your financial support is greatly appreciated as it allows me to devote what is often large amount of time I spend researching and writing my posts, so again, thanks. - Pierre
“Shedding” Part 1- Shedding of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated - Part 1
“
Shedding” Part 2 - The Bio-Distribution and Excretion Potential of Covid mRNA Vaccine Products
“
Shedding” Part 3 - Can You Absorb Lipid Nanoparticles From Being Exposed To a Vaccinated Person?
“
Shedding” Part 4 - Evidence of Placental and Breast Milk Transmission of Covid mRNA Vaccine Components
"
Shedding" Part 5 - Evidence of Shedding Causing Illness In Others
“
Shedding Part 6- Clinical Case Notes Describing Shedding Phenomena Among Leading Edge Clinic Patients
“
Shedding” Part 7 - Shedding Via Sexual Intercourse - Clinical Reports
“
Shedding” Part 8 - A Deluge of Clinic Reports Pour In


