https://pierrekorymedicalmusings.com/p/shedding-part-2-the-bio-distribution"
Shedding Part 2- The Bio-Distribution and Excretion of Covid mRNA Vaccine Components and ProductsIn order to transmit or "shed" the Covid mRNA encapsulated lipid nanoparticle and/or the transcribed spike protein product, dissemination to organs and body fluids must occur. Does it? Answer: Yes.
Pierre Kory, MD, MPA
Nov 1, 2023
OK, so in Part 1 of this series on Covid mRNA vaccine shedding, I provided evidence that:
The FDA and the EMA define the mRNA vaccines as gene therapies.
The FDA requires that gene therapy products undergo human shedding studies given the known risks of shedding
Shedding studies were not done because, even though the vaccines are gene-therapies, they legally fell under the legal definition of a “countermeasure” in a public health emergency. Countermeasures do not require shedding or other types of safety studies before mass use.
All we know is that from a FOIA obtained document, Pfizer did a shedding study on rats but we don’t know what they found.
HOW DOES SHEDDING OCCUR AND IS THERE ANY EVIDENCE OF IT OCCURRING WITH THE COVID mRNA VACCINES?
In order for the vaccine or spike to be shed, it would first require distribution of the vaccine components or spike protein product to the lungs (to then be exhaled) and other body fluids (to then be excreted)
To explore this possibility, it is important that we define what a lipid nanoparticle LNP) is, along with their natural, biological counterparts which are called exosomes or extracellular vesicles (EVs).
The papers I reviewed used the terms exosomes, LNP’s, EV’s, and even nanoparticles somewhat interchangeably although there are some differences. For instance, exosomes are a subset of extracellular vesicles (EV’s). From this paper in Molecular Therapy, they state:
Exosome-like nanovesicles (ELNVs) are biological nanostructures of 40–150 nm, are secreted by most types of cells and relay information between cells and organisms across all three kingdoms of life.1,2 Although earlier perceived to be cellular debris and hence undervalued, ELNVs are now acknowledged as crucial entities to regulate physiological functions of multicellular organisms in an intercellular transmission manner.
From another paper in Science:
Exosomes are EVs with a size range of ~40 to 160 nm (average ~100 nm) in diameter with an endosomal origin. For instance, the LNP’s in the Covid MRNA vaccines are approximately 100 - 400 nm in size.
The most important fact to remember is that the smaller the size, the more widely they distribute and the more easily they can enter the body (more on the latter later).
For context, the length of the SARS-Cov2 virus is about 9-12 nm in size. Further, as Banoun points out in her masterful review of the topic of shedding:
“Huge amounts of mRNA are injected compared to the circulation of a virus during a natural infection: up to 10 to 7 times more, according to Professor Jean-Michel Claverie [27].”
Further, there are different biologic materials that can be used to make the outer membrane enclosing the contents of a nanoparticle. Lipids (i.e. liposomes or LNP’s) are one of the most commonly used for drug delivery. Early conventional “liposomes” (yet another term) had limitations such as short half-life and rapid systemic clearance following their clearance by the reticuloendothelial system (RES). However, the conjugation of polymers such as polyethylene glycol (PEG) resulted in the generation of sterically stabilized liposomes with prolonged half-life and increased stability.
To wit, the Covid mRNA vaccines used PEG to stabilize the LNP carrying the modified mRNA.
So what are nanoparticles/LNPs/exosomes, what is inside them, and what do they do?
Basically, they are tiny sacs enclosed by a lipid membrane which can contain any of the following: proteins, metabolites, enzymes, growth factors, and nucleic acids. You can also package drugs (and synthetic mRNA) into them in order to deliver their contents into recipient cells to effectively alter their biological response.
Natural, endogenous exosomes are associated with immune responses, viral pathogenicity, pregnancy, cardiovascular diseases, central nervous system–related diseases, and cancer progression. Such exosome-mediated responses can be disease promoting or restraining. Exosomes can be engineered to deliver diverse therapeutic payloads, including short interfering RNAs, antisense oligonucleotides, chemotherapeutic agents, and immune modulators, with an ability to direct their delivery to a desired target.
Importantly, synthetic mRNA vaccine LNPs have the same structure as the natural exosomes they seek to mimic.
So what do we know about human biodistribution of synthetic LNP’s??
From this article by Sonia Elijah, regulators knew LNP’s distribute widely in the human body:
In the recent leaked letter by the EMA, Executive Director, Emer Cooke, to the Chair of COVID-19 Special Committee, MEP Kathleen Van Brempt, Cooke begrudgingly admitted, “that the lipid nanoparticles can distribute rather non-specifically to several organs such as liver, spleen, heart, kidney, lung and brain, with the liver appearing to be the organ where the lipid nanoparticles distribute most.”
Her admission was made on the heels of the Therapeutics Goods Administrations (TGA) of Australia’s evaluation report on Pfizer’s nonclinical biodistribution study, which alarmingly revealed that the lipid nanoparticles which encase the mRNA, travel to the liver, spleen, brain, eyes, bone marrow, adrenal glands, ovaries and testes– nearly every organ tissue.
Further, beyond the mRNA encased in synthetic LNP’s, “naked” mRNA as well as mRNA encased in natural LNP’s (called exosomes) and spike protein in free form or encapsulated in exosomes can be found in the bloodstream and breast milk.
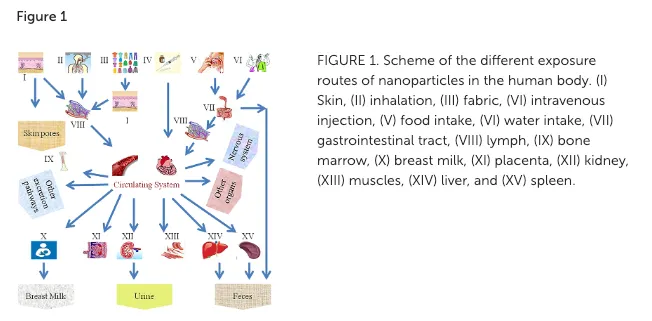
More worryingly, LNP’s or their natural equivalent, exosomes (a.k.a. extracellular vesicles (EVs)) are able to be excreted through body fluids (sweat, sputum, breast milk) and to pass the transplacental barrier. These exosomes are also able to penetrate by inhalation and through healthy or injured skin as well as orally through breast milk.
This figure from a review paper on nanoparticle therapies is illuminating:

much, much, more
https://pierrekorymedicalmusings.com/p/shedding-part-2-the-bio-distributionhttps://pierrekorymedicalmusings.com/p/shedding-part-3-can-you-absorb-lipid?"Shedding Part 3 - Can You Absorb Lipid Nanoparticles From Being Exposed To a Vaccinated Person?I review all the routes of entry into the human body that mRNA vaccine nanoparticles can take.. and the ease in which they do so.
The most troubling is via inhalation.Pierre Kory, MD, MPA
Nov 1, 2023
In this post, I will review the ways in which the synthetic lipid nanoparticles (LNPs), used in the Covid mRNA vaccines (as well as natural LNPs called exosomes) can be absorbed into the body.
First, a summary of the data presented in my first 2 posts
here and
here:
The Covid mRNA vaccines meet the regulatory definition of a gene therapy product
Gene therapy products are required to undergo both animal and human shedding studies (the latter were not done and the results of the former have not been made public by Pfizer).
Shedding studies are required because the mRNA is delivered to the cell via lipid nano-particles and LNP’s are distributed widely in the body
Pfizer specifically excluded subjects who could be closely exposed to a trial subject that had already received the vaccine.
The gene therapy product called Luxterna has a warning on its insert that the product can be shed via tears and nasal secretions.
Where is the evidence that LNP’s from vaccinated folks can be transmitted to and subsequently enter our bodies? From this review of nanoparticles (i.e LNPs/exosomes) they state:
As far as the exposure of humans to NPs is concerned, they can enter the body through inhalation, ingestion, skin uptake, injection, or implantation. It is also interesting to note that NP uptake could be intentional or non-intentional.
Non-intentional? From the article: “Some exposures are unintentional, such as pulmonary inhalation of NPs in the environment or at manufacturing sites.”
This figure illustrates the various routes of absorption and dissemination throughout the body:
Here is where we are: synthetic LNP’s like the Covid vaccines contain modified mRNA. Natural exosomes can take up released modified mRNA as well as the spike protein. LNP’s and exosomes distribute widely throughout the body. But can they be released from the body? If released via body fluids or exhaled breath, can they then be absorbed by others who are exposed to these fluids/vapor?
A major concern is that this study found that vaccine mRNA is present from day one and persists in the bloodstream for at least 2 weeks after injection; its concentration starts to decrease after 4 days. Note this is much longer than was claimed by the manufacturers on the basis of brief studies in rats.
From the conclusion of the study:
In conclusion, we showed that BNT162b2 vaccine mRNA remains in the systemic circulation of vaccinated individuals for at least 2 weeks, during which it likely retains its ability to induce S-protein expression in susceptible cells and tissues.
So mRNA can stay in the blood for up to two weeks. However, in my now almost two year clinical experiences treating both Long Vax and Long Covid, it is clear that the spike protein is the most worrisome given its severe pathogenicity and toxicity.
Let’s start with what we know about distribution of spike protein to organs and body fluids (this would be required in order to support the fact that shedding can occur):
In July of 2021 a page on the website of the Infectious Disease Society of America noted that the lifespan of spike in the bloodstream is “unknown and may be a few weeks.” That page no longer exists. This might be because of the publication of numerous studies showing not only wide dissemination but also the persistence of spike protein in the body:
For example, this research team reported that the spike protein persists for a long time in free form: full-length spike is detected up to day 15, with a peak at 62 pg/mL. After the 2nd dose, free spike is no longer detected as it would be bound to antibodies (but the study did not look for antibody-spike immune complexes).
Another study found that vaccination with mRNA and translation of the mRNA induces the production of exosomes carrying the spike protein and circulating in the blood 14 days after injection and up to 4 months after.
Another group similarly found that the spike protein concentration rapidly increases in blood after vaccination (within 1 to 3 days) and persists in the bloodstream for more than a week. Although they report that the spike is completely eliminated within 1 month a more recently published study which looked much more carefully, found spike protein circulating in the blood up to 187 days after vaccination (after which they stopped testing and finished their study).
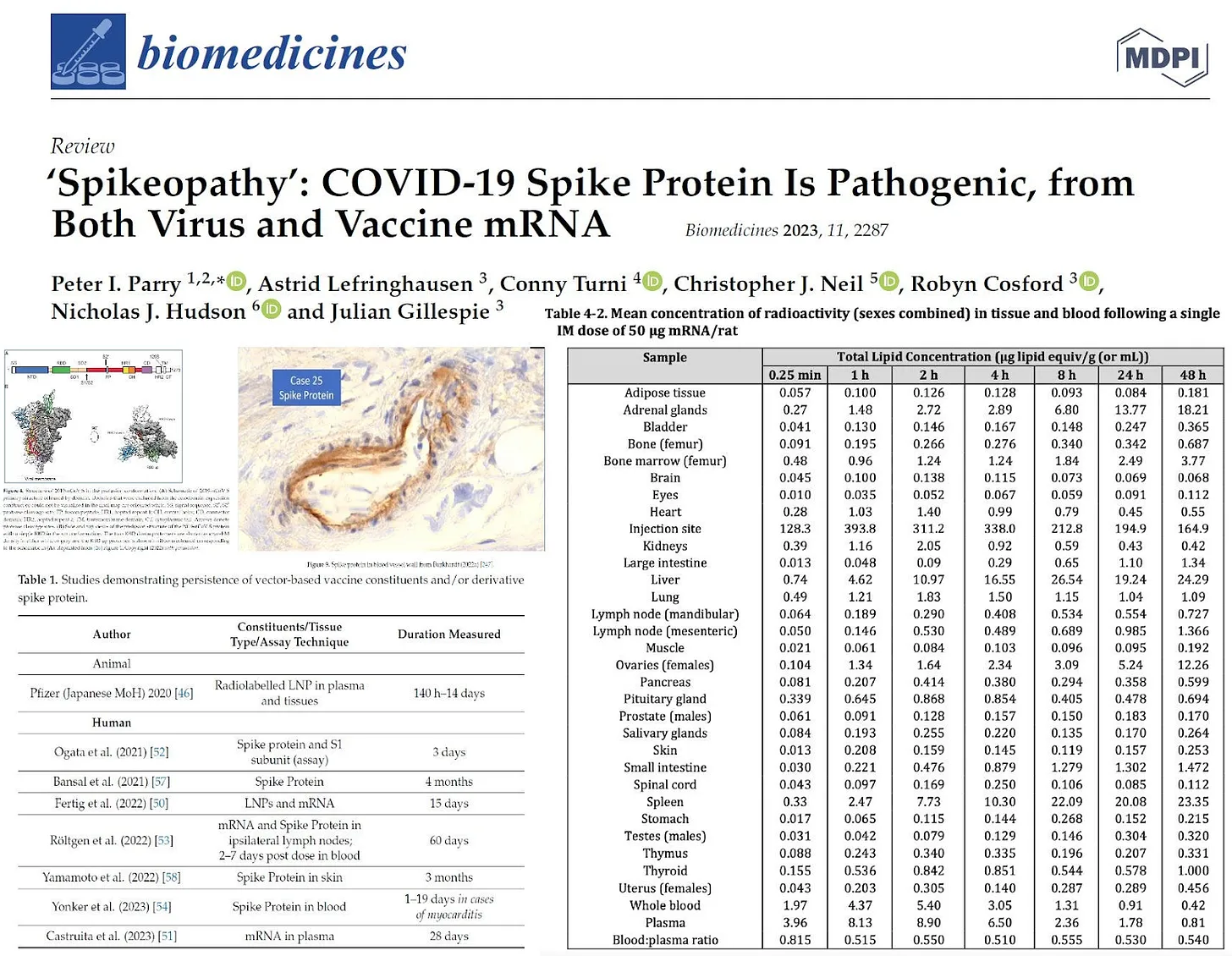
In the Parry et al review paper on “spikeopathy”, they include a table summarizing the persistence of various vaccine products in various organs as in the below bottom left (image taken from William Makis’s review of the paper on his Substack called Covid Intel):
Clinical and pathologic evidence abound as well: a case report of an autopsy done in a man who died of multifocal necrotizing encephalitis three weeks after the vaccine found vaccine spike in numerous organs (heart, brain, muscles, germinal centers etc.). Further, they emphasized the finding of high concentrations in the walls of capillaries. One sentence in that report jumped out at me:
“The family of the deceased requested an autopsy due to ambiguous clinical signs before death.”
That is exactly the patient population autopsied by a team of pathologists led by senior German pathologist Arne Burkhart (unfortunately he is recently deceased but many of us Covid dissidents co-lectured at conferences with him - he was a brilliant, courageous, and kind man).
Know that in order to establish the vaccine as the cause of death on autopsy, you have to use a special stain to identify the spike protein embedded in the organs or vessels, something that nearly all “system” coroners across the world did NOT do. As the independent pathologist Ryan Cole has said “you can’t find what you don’t look for.” It was clear to all of us Covid “dissidents” that from the outset there was a concerted, global effort to avoid looking for disseminated spike protein in the bodies of the deceased.
This is why the findings of Burkhart’s team are so alarming (and censored) They began systematically performing “2nd opinion” autopsies staining for the presence of spike protein in people who died where the family was convinced the vaccine was the cause (and the primary coroner had not performed these special stains).
Although not yet published, he has presented their findings in multiple invited lectures. He reported that out of the first 50 autopsies performed, in 80% of cases where the family suspected the vaccine as the cause of death, spike induced organ damage was determined to be the proximate cause of death.
In that lecture, Burkhart showed slides of properly stained tissues demonstrating not only widespread dissemination of the spike protein, but also widespread spike-induced damage to tissues and vessels (i.e. vessel walls, heart muscle, brain tissue, kidneys etc).
More recently, another group of publicly vocal Covid “dissident” scientists including Peter McCullough, Harvey Risch, Mark Trozzi, and others performed a systematic review of autopsies where the spike protein was stained for. The spike was found to be the cause of death in 74% of cases. Unsurprisingly, the paper was nearly immediately retracted off of a… pre-print server. It just doesn’t stop.
So, LNPs, naked mRNA, naked spike and spike containing exosomes are disseminated in the bloodstream and to tissues as long as 187 days from vaccination (know this is not a limit, it is just the longest they followed the patient for). The dissemination of spike protein can cause immense organ damage leading to death.
Now, are the vaccine product containing exosomes/LNP’s capable of being transmitted (“shed”) and then absorbed by the bodies of unvaccinated individuals in contact with freshly vaccinated individuals? In this paper they state:
much, much, more
https://pierrekorymedicalmusings.com/p/shedding-part-3-can-you-absorb-lipid?


