This post was actually copy and pasted on
6-12-2021 (contrary to the post dating at the top of this post, I pasted it in an old "bump" post).
The NIH non-recommendations are largely the same as they have been all along. In other words, if don't opt for early outpatient treatment with hydroxychloroquine or ivermectin protocols, your odds are much greater of dying under the "standard of care" in a hospital.
The only exception I noticed in the recommendations for perhaps over a year now, was prescribing monoclonal antibodies earlier for higher risk patients.
And what does it cost? $1,250 per vial
https://www.globaldata.com/eli-lillys-covid-19-mab-bamlanivimab-potential-cost-effectiveness-underscores-payer-support/As has become typical: "PulmCrit Wee – Follow-up
Bamlanivimab study unmasks statistical chicanery"
"Whether or not you have any interest in bamlanivimab, you should read this post as an amusing example of shoddy statistics being published in top journals."
https://emcrit.org/pulmcrit/followup-bamlanivimab/Meanwhile, earlier in this forum section we find doctors that have been having 100% success in treatment of their elderly and high-risk patients for well over a year and a half now, with hydroxychloroquine+azithromycin+zinc or ivermectin+doxycycline+zinc. Both costing less than $20 for the complete protol.
Therapeutic Management of Adults With COVID-19
Last Updated: May 24, 2021
Executive Summary
Two main processes are thought to drive the pathogenesis of COVID-19. Early in the clinical course, the disease is primarily driven by replication of SARS-CoV-2. Later in the clinical course, the disease appears to be driven by a dysregulated immune/inflammatory response to SARS-CoV-2 that leads to tissue damage. Based on this understanding, it is anticipated that antiviral therapies would have the greatest effect early in the course of the disease, while immunosuppressive/anti-inflammatory therapies are likely to be more beneficial in the later stages of COVID-19.
No therapy has been proven to be beneficial in outpatients with mild to moderate COVID-19 who are not at high risk for disease progression.
Which is the same deadly lie they have been telling since March of 2020 thereby advancing Big Pharma profits ever since March of last year - that resulted in the needless deaths of well over half a million Americans and millions worldwide - even as hydroxychloroquine and ivermectin were demonstrating themselves to be up to 100% effective across all groups ever since March of 2020. While the NIH has been recommending nothing until a patient begins to suffocate and needs oxygen.
This even though
Fauci and his NIH established back in 2005 that hydroxychloroquine is highly effective both as prophylaxis and in therapeutic treatment of SARS corona viruses.
https://www.covid-19forum.org/index.php?topic=399.0The COVID-19 Treatment Guidelines Panel (the Panel) recommends providing supportive care and symptomatic management to outpatients with COVID-19; steps should also be taken to reduce the risk of SARS-CoV-2 transmission to others.1,2 Patients should be advised about when to seek in-person evaluation. See Outpatient Management of Acute COVID-19 for more information.
In outpatients with mild to moderate COVID-19 who are at high risk for disease progression, anti-SARS-CoV-2 antibody-based therapies may have the greatest potential for clinical benefit during the earliest stages of infection. For these patients, the Panel recommends administering bamlanivimab plus etesevimab (AIIa) or casirivimab plus imdevimab (AIIa), both of which are available through Emergency Use Authorizations (EUAs) from the Food and Drug Administration (FDA). See Anti-SARS-CoV-2 Monoclonal Antibodies for more information about using these combinations and other monoclonal antibodies.
Remdesivir, an antiviral agent, is currently the only drug that is approved by the FDA for the treatment of COVID-19. It is recommended for use in hospitalized patients who require supplemental oxygen. However, it is not routinely recommended for patients who require mechanical ventilation due to the lack of data showing benefit at this advanced stage of the disease.3-6
The WHO sponsored a study that was conducted from March 22 to Oct. 4 and involved 11,330 patients from 405 hospitals in 30 countries.
They found no statistically significant reduction in mortality, or even reduction in the length of hospital stay which is all an earlier useless manipulated NIH study had credited it with.
https://www.covid-19forum.org/index.php?topic=367.0So of course the WHO later conditionally recommended against the use of Remdesivir. Little surprise then, just days later, the FDA formally approved that dangerous and less effective drug.
https://www.covid-19forum.org/index.php?topic=448.0Dexamethasone, a corticosteroid, has been found to improve survival in hospitalized patients who require supplemental oxygen, with the greatest benefit observed in patients who require mechanical ventilation. Therefore, the use of dexamethasone is strongly recommended in this setting.7-10
Corticosteroids are effective (particularly when combined in a multi-drug therapy with ivermectin as shown in the original post) in treating the later inflammatory stage of COVID, which is where a patient winds up if their physician failed to treat them early with the $20 HCQ or ivermectin treatment protocols. But even with this NIH recommendation, according to Dr. Peter McCullough his patients "languished on dexamethasone" but responded better to prednisone.
Adding tocilizumab, a recombinant humanized anti-interleukin-6 receptor monoclonal antibody, to dexamethasone therapy was found to improve survival among patients who were exhibiting rapid respiratory decompensation due to COVID-19.11,12
The Panel continues to review the most recent clinical data to provide up-to-date treatment recommendations for clinicians who are caring for patients with COVID-19.
Then why didn't they make recommendations based on the clinical data of successful treating physicians that have cured tens of thousands of patients over the last 1-1/2 year with HCQ and ivermectin? Like those in this forum section such as Dr. Zelenko, Dr. Tyson and Dr.s Ratier?
Why didn't they review the 96 ivermectin studies, 58 peer reviewed, 58 with results comparing treatment and control groups. With
97% of 37 early treatment and prophylaxis studies reporting positive effects and 95% of all 58 studies showing the same.
https://c19ivermectin.com/Why didn't they review the 305 hydroxychloroquine studies, 224 peer reviewed, 255 comparing treatment and control groups, with
100% of the 29 early treatment studies demonstrating positive effect?
Figure 1 summarizes the Panel’s recommendations for managing patients with varying severities of disease.
Recommendations for Pharmacologic Management of Patients with COVID-19 Based on Disease Severity
For definitions of the clinical severity categories for patients with COVID-19, please see Clinical Spectrum of SARS-CoV-2 Infection.
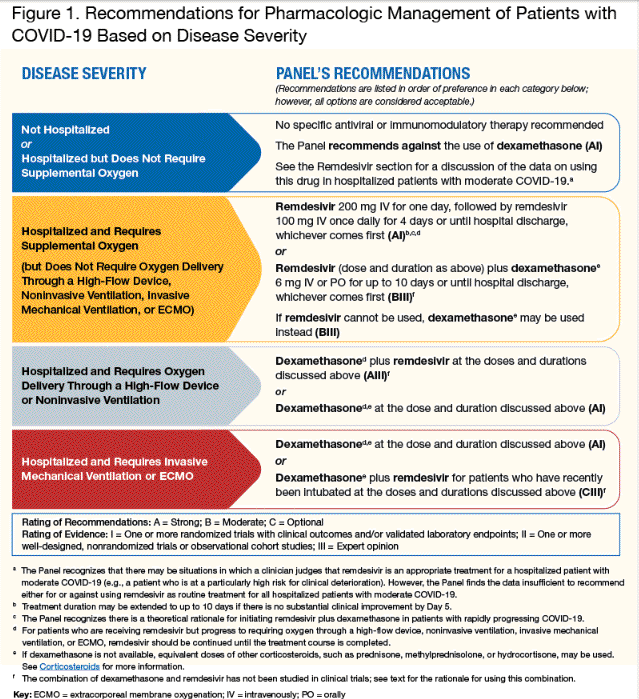
"Not hospitalized or hospitalized but does not require supplemental oxygen" - "No specific antiviral or immunomodulatory therapy recommended". That absence of recommendations, accompanied by Big Pharma's lackeys in government and media demonizing effective early treatment protocols that utilize HCQ and IVM along with competent doctors that prescribed them, is directly responsible for the homicide of a million Americans and millions more worldwide through negligence and malpractice, whose governments trusted Fauci's deadly U.S. lead. Postponing any effective treatment allowing the virus to replicate wildly and out of control until the disease advances into the pulmonory phase and the patient begins to suffocate.
Now compare the green arrow no outpatient recommendations portion of that chart with the early outpatient treatment chart of recommendations in from the FLCCC.
Patients With Mild to Moderate COVID-19 Who Are Not Hospitalized
Recommendations
For patients who are not at high risk of disease progression:
The Panel recommends providing supportive care and symptomatic management (AIII).
For patients who are at high risk of disease progression, as defined by the EUA criteria for treatment with anti-SARS-CoV-2 monoclonal antibodies:
The Panel recommends using one of the following combination anti-SARS-CoV-2 monoclonal antibodies (treatments are listed in alphabetical order):
Bamlanivimab 700 mg plus etesevimab 1,400 mg (AIIa); or
Casirivimab 1,200 mg plus imdevimab 1,200 mg (AIIa).
Treatment should be started as soon as possible after the patient receives a positive result on a SARS-CoV-2 antigen test or a nucleic acid amplification test and within 10 days of symptom onset.
When risking toxic chemicals produced by Big Pharma, it would be a good idea to wait until you get a positive test,
except for the fact that they are next to worthless. So making a decision based on waiting on the results of a PCR test could use up at least some of the early treatment window. That's why colleagues from 7 universities are suing the CDC for fraud, after looking at 1500 supposedly positive COVID-19 tests with an electron microscope and finding absolutely no COVID-19 viruses but only influenza A and B.
https://www.covid-19forum.org/index.php?topic=747.0Did anybody really wonder why the seasonal flu was down 98% this year, at the same time that another virus was raging on? How stupid do they think we are?
https://www.covid-19forum.org/index.php?topic=657.0False negatives are even worse. A neighbor's mother and father got tested. She tested positive and got treated, while he tested negative 5 times that delayed treatment and he died, but not before suffering on a ventilator for some time.
No surprise when the PCR test produces false negatives at the rate of 67% even at day 4!
https://www.covid-19forum.org/index.php?topic=698.0Blessedly, the ivermectin and hydroxychloroquine protocols are so safe, they are generally administered upon the presentation of symptoms or even just clinical suspicion of COVID-19. After all, millions of Americans take hydroxychloroquine every day of the year over decades for Lupus and rheumatoid arthritis, in the same dosage that the COVID treatment protocols prescribe over just 7 days.
Additional Considerations
There are no comparative data to determine whether there are differences in clinical efficacy or safety between bamlanivimab plus etesevimab and casirivimab plus imdevimab.
There are SARS-CoV-2 variants, particularly those that contain the mutation E484K, that reduce the virus’ susceptibility to bamlanivimab and, to a lesser extent, casirivimab and etesevimab in vitro; however, the clinical impact of these mutations is not known.
The availability of bamlanivimab plus etesevimab may be restricted in areas with an elevated prevalence of variants of concern that have markedly reduced in vitro susceptibility to these agents (e.g., P.1, B.1.351). Please visit this website from the Department of Health and Human Services for updates on the distribution of bamlanivimab plus etesevimab and the Centers for Disease Control and Prevention’s website for information on the proportions of SARS-CoV-2 variants.
In regions where SARS-CoV-2 variants of concern or interest with modestly reduced in vitro susceptibility to bamlanivimab plus etesevimab are common (e.g., B.1.526), some Panel members would preferentially use casirivimab plus imdevimab while acknowledging that it is not known whether in vitro susceptibility data correlate with clinical outcomes.
Rationale for Recommending Supportive Care and Symptomatic Management for Patients Who Are Not at High Risk of Disease Progression
No specific therapy has been proven to be beneficial in outpatients with mild to moderate COVID-19 who are not at high risk for disease progression.
The same old lie they've been peddling since spring of 2020. Even Tamiflu can help if taken within the first two days of symptoms. The $20 treatment protocols will benefit anyone who is symptomatic for COVID-19 at any age. They are just unnecessary for most healthy younger people with sufficient vitamin C and D levels because COVID should not be much of an event for them. According to competent treating physicians everyone and anyone that becomes short of breath should get on one of the $20 treatment protocols. And ivermectin has demonstrated efficacy through all stages of the disease.
The Panel recommends supportive care and symptomatic management (AIII), with close monitoring for worsening symptoms and clinical deterioration for patients.
Rationale for the Use of Combination Anti-SARS-CoV-2 Monoclonal Antibodies
Two anti-SARS-CoV-2 combination products—bamlanivimab plus etesevimab and casirivimab plus imdevimab—have received EUAs from the FDA for the treatment of outpatients with mild to moderate COVID-19 who are at high risk of disease progression (as defined by the EUA). The FDA had previously issued an EUA for bamlanivimab alone. Due to the increase in circulating variants that have the potential for resistance to bamlanivimab, that EUA has since been revoked.
Several circulating SARS-CoV-2 variants, particularly those that contain the mutation E484K, are associated with reduced susceptibility to bamlanivimab and, to a lesser extent, casirivimab and etesevimab in vitro.
While Dr. Pierre Kory indicated that ivermectin should have excellent efficacy against the variants, and so should the natural immunity one gets from having had COVID.
https://www.bitchute.com/video/a3a0EOIe8aK1/However, the clinical impact of these mutations is not known. Reduced in vitro susceptibility to both antibodies in a combination regimen is currently uncommon. Please see Anti-SARS-CoV-2 Monoclonal Antibodies for more information regarding the circulating SARS-CoV-2 variants of concern and interest and the susceptibility of these variants to anti-SARS-CoV-2 monoclonal antibodies.
The clinical trial data that demonstrate the clinical benefit of these anti-SARS-CoV-2 monoclonal antibody combinations for the treatment of outpatients with mild to moderate COVID-19 are outlined below. It is worth noting that these studies were conducted before the widespread circulation of the variants of concern.
Clinical Data
Bamlanivimab Plus Etesevimab
The EUA for bamlanivimab plus etesevimab was based on data from several studies, including the Blocking Viral Attachment and Cell Entry With SARS-CoV-2 Neutralizing Antibodies (BLAZE)-1 and BLAZE-4 trials.
In the Phase 3 BLAZE-1 trial, a randomized trial that included 1,035 high-risk participants, the primary endpoint was the proportion of participants who had a COVID-19-related hospitalization (defined as ≥24 hours of acute care) or who died from any cause by Day 29. Compared to those who received placebo, participants who received bamlanivimab 2,800 mg plus etesevimab 2,800 mg had a 5% absolute reduction and a 70% relative reduction in COVID-19-related hospitalizations or death from any cause; endpoint events occurred in 11 of 518 participants (2.1%) in the bamlanivimab plus etesevimab arm and in 36 of 517 participants (7.0%) in the placebo arm (P = 0.0004). There were no deaths in the bamlanivimab plus etesevimab arm, and 10 deaths occurred in the placebo arm.13,14
"PulmCrit Wee – Follow-up Bamlanivimab study unmasks statistical chicanery"
"Whether or not you have any interest in bamlanivimab, you should read this post as an amusing example of shoddy statistics being published in top journals."
https://emcrit.org/pulmcrit/followup-bamlanivimab/Of note, the doses authorized in the EUA (bamlanivimab 700 mg plus etesevimab 1,400 mg) are different from the doses studied in the Phase 3 BLAZE-1 study. The available data suggest that the antiviral activity of this lower dose is similar to that of bamlanivimab 2,800 mg plus etesevimab 2,800 mg.14
Casirivimab Plus Imdevimab
The recommendation for the use of casirivimab plus imdevimab is based on Phase 3 results from the R10933-10987-COV-2067 study (the information from this study is currently available only in a press release, and there is no peer-reviewed preprint or publication).15 This trial compared 1,355 participants who received casirivimab 1,200 mg plus imdevimab 1,200 mg to 1,341 participants who received placebo.
The modified full analysis set included participants who were aged ≥18 years and had a positive SARS-CoV-2 polymerase chain reaction result from a nasopharyngeal swab at randomization and one or more risk factors for severe COVID-19. COVID-19-related hospitalizations or death from any cause were reported in 18 of 1,355 participants (1.3%) in the casirivimab plus imdevimab arm and in 62 of 1,341 participants (4.6%) in the placebo arm (P < 0.0001). This represents a 3.3% absolute reduction and a 71% relative reduction in hospitalization or death in the casirivimab plus imdevimab treatment participants.
Patients Who Are Hospitalized With Moderate COVID-19 but Who Do Not Require Supplemental Oxygen
Recommendations
The Panel recommends against the use of dexamethasone or other corticosteroids (AIIa). Patients who are receiving dexamethasone or another corticosteroid for other indications should continue therapy for their underlying conditions as directed by their health care provider.
There are insufficient data to recommend either for or against the routine use of remdesivir in these patients. The use of remdesivir may be appropriate in patients who have a high risk of disease progression.
Rationale for Recommending Against the Use of Dexamethasone or Other Corticosteroids
In the Randomised Evaluation of COVID-19 Therapy (RECOVERY) trial, a multicenter, open-label trial in the United Kingdom, hospitalized patients with COVID-19 were randomized to receive either dexamethasone plus standard of care or standard of care alone (control arm).7 In the subgroup of participants who did not require supplemental oxygen at enrollment, no survival benefit was observed for dexamethasone: 17.8% of participants in the dexamethasone arm and 14% in the control arm died within 28 days of enrollment (rate ratio 1.19; 95% CI, 0.91–1.55). Please see Table 4a for additional information. Based on these data, the Panel recommends against the use of dexamethasone (AIIa) or other corticosteroids (AIII) for the treatment of COVID-19 in this subgroup, unless the patient has another indication for corticosteroid therapy.
Rationale for the Panel’s Assessment That There Are Insufficient Data to Recommend Either for or Against the Use of Remdesivir
The Adaptive COVID-19 Treatment Trial (ACTT-1) was a multinational randomized controlled trial that compared remdesivir to placebo in hospitalized patients with COVID-19. Remdesivir showed no significant benefit in patients with mild to moderate disease, which was defined as oxygen saturation >94% on room air or a respiratory rate <24 breaths/min without supplemental oxygen (rate ratio for recovery 1.29; 95% CI, 0.91–1.83); however, there were only 138 patients in this group.3
In a manufacturer-sponsored, open-label randomized trial of 596 patients with moderate COVID-19, patients who received 5 days of remdesivir had higher odds of having a better clinical status on Day 11 (based on distribution on a seven-point ordinal scale) than those who received standard of care (OR 1.65; 95% CI, 1.09–2.48; P = 0.02). However, the difference between the groups was of uncertain clinical importance.5
The Solidarity trial was a large, multinational, open-label randomized controlled trial.....
Same study they administered toxic doses of hydroxychloroquine to the unwitting participants in, to make it appear dangerous, even after a 65-year history of safety and billions of doses having been prescribed with little side effect - particularly when compared to so many deadly drugs that the Big Pharma industry criminals crank out.
https://www.covid-19forum.org/index.php?topic=105.0.....in which a 10-day course of remdesivir was compared to standard of care. About 25% of hospitalized patients in the remdesivir and control arms did not require supplemental oxygen at study entry. The primary outcome of in-hospital mortality occurred in 11 of 661 patients (2%) in the remdesivir arm and in 13 of 664 patients (2.1%) in the control arm (rate ratio 0.90; 99% CI, 0.31–2.58).16 The open-label design of this study makes it difficult to determine whether remdesivir affects recovery time as determined by duration of hospitalization, because patient discharge may have been delayed in order to complete remdesivir therapy. Please see Table 2a for additional information.
Because these trials produced conflicting results regarding the benefits of remdesivir, the Panel finds the available data insufficient to recommend either for or against routine treatment with remdesivir for all hospitalized patients with moderate COVID-19. However, the Panel recognizes that there may be situations in which a clinician judges that remdesivir is an appropriate treatment for a hospitalized patient with moderate disease (e.g., a person who is at a particularly high risk for clinical deterioration).
For Hospitalized Patients With COVID-19 Who Require Supplemental Oxygen but Who Do Not Require Oxygen Delivery Through a High-Flow Device, Noninvasive Ventilation, Invasive Mechanical Ventilation, or Extracorporeal Membrane Oxygenation
Recommendations
The Panel recommends one of the following options for these patients:
Remdesivir (e.g., for patients who require minimal supplemental oxygen) (BIIa);
Dexamethasone plus remdesivir (e.g., for patients who require increasing amounts of oxygen) (BIII); or
Dexamethasone (e.g., when combination therapy with remdesivir cannot be used or is not available) (BI).
That's it! Now look at the multi-drug therapy that the FLCCC outlines in the original post. Doing everything a doctor can to keep a patient out of the hospital and subsequent risk of death.
Additional Considerations
Certainly nothing redeeming in this section.


