We can smell the palpable fear as Big Pharma's
information laundering services - medical journals - will apparently publish any amount of propaganda in their continuing effort to blow a smokescreen over Big Pharma's/government's/media's mass homicide of over a million Americans and millions more worldwide in their continuing crimes against humanity.
One of Big Pharma's propaganda ministries, JAMA published an article that condemns
highly successful actual front line treating physicians - that have been nearly 100% successful in early treatment of all of their COVID patients since the spring of 2020 - as propagating misinformation that has been the reason that Americans have died. So let's explore it in a little more detail.
First about journals, as former editors put it regarding Big Pharma's captured medical journals (Pharma provides up to 98% of ad revenue):
"Consider Dr. Richard Horton of the medical journal, Lancet, who once wrote:
“
Journals have devolved into information-laundering operations for the pharmaceutical industry.”
Or how about this frank observation from Dr. Marcia Angell:
“
It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines."
“I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.”""Medical journals: “information-laundering for Big Pharma”?"On to the JAMA article I found posted on Twitter:
https://twitter.com/jonathanstea/status/1691529420375556096August 15, 2023
Communication of COVID-19 Misinformation on Social Media by Physicians in the US
Sahana Sule, BS1; Marisa C. DaCosta, BS1; Erin DeCou, MPA1; et al
Quite the powerhouse. A couple with BS degrees, a master of public administration, a master of public health and an MD. Something tells me they should have consulted attorneys before engaging in their defamation. Or is that the reason they failed to post the names of the 52 physicians they lied about engaging in misinformation rendering their creation moot?
Meet a few of the medical professionals that we rely on for forum informationKey Points
Question
What types of COVID-19 misinformation have been propagated online by US physicians and through what channels?
Findings
In this mixed-methods study of high-use social media platforms, physicians from across the US and representing a range of medical specialties were found to propagate COVID-19 misinformation about vaccines, treatments, and masks on large social media and other online platforms and that many had a wide reach based on number of followers.
Interesting how some with BS degrees and others apparently not even that, would appoint themselves arbiters of what is and is not "misinformation", that they lie about being propagated by
actual front line treating physicians that have been in the front lines of successful COVID treatment since the beginning of the pLandemic.
Meaning
This study’s findings suggest a need for rigorous evaluation of harm that may be caused by physicians, who hold a uniquely trusted position in society.....
But no longer trust the negligent doctors that allowed their patients to suffer severe COVID and resulting death and long-COVID, through their medical malpractice by having deprived their patients of near perfect early treatment at home with $20 HCQ or IVM generic drug/nutraceutical protocols.
.....propagating misinformation; ethical and legal guidelines for propagation of misinformation are needed.
Needed indeed, beginning with the harm caused by Big Pharma's misinformation propagandists - such as the authors of this article - as will become apparent. Pharma's liars that were in full swing by the time
The Lancet published the fraudulent "study" with fictional data on hydroxychloroquine - that was withdrawn within a couple weeks - that Pharma's captured media disinformation liars nonetheless continued to propagate for years are guilty of negligent homicide at best and crimes against humanity. Pretending that HCQ is dangerous, even though millions of Americans were taking it every day of the year, decade after decade for rheumatoid arthritis and Lupus, in the same dosage that COVID treatment protocols prescribe over just 7 days. Is there much that demonstrates how Pharma's minions lied more than that? Unfortunately there's lots more that demonstrates it.
Abstract
Importance
Approximately one-third of the more than 1 100 000 confirmed COVID-19–related deaths as of January 18, 2023, were considered preventable if public health recommendations had been followed. Physicians’ propagation of misinformation about COVID-19 on social media and other internet-based platforms has raised professional, public health, and ethical concerns.
THE REALITY is exactly the opposite of that LIE. Over a million Americans are
in their graves specifically BECAUSE THEY FOLLOWED PUBLIC HEALTH RECOMMENDATIONS. Like Fauci's "go home and iosolate" with no treatment recommendations until you began to suffocate, then go to the hospital and get
poisoned by Remdesivir (even though at the same time highly successful front line
treating physicians were enjoying near 100% success in treatment of high-risk patients, from March of 2020 onward).
Fauci's "go home and isolate" treatment for COVID - a death sentence for some NIH deadly recommendations compared to those of COVID-competent professionals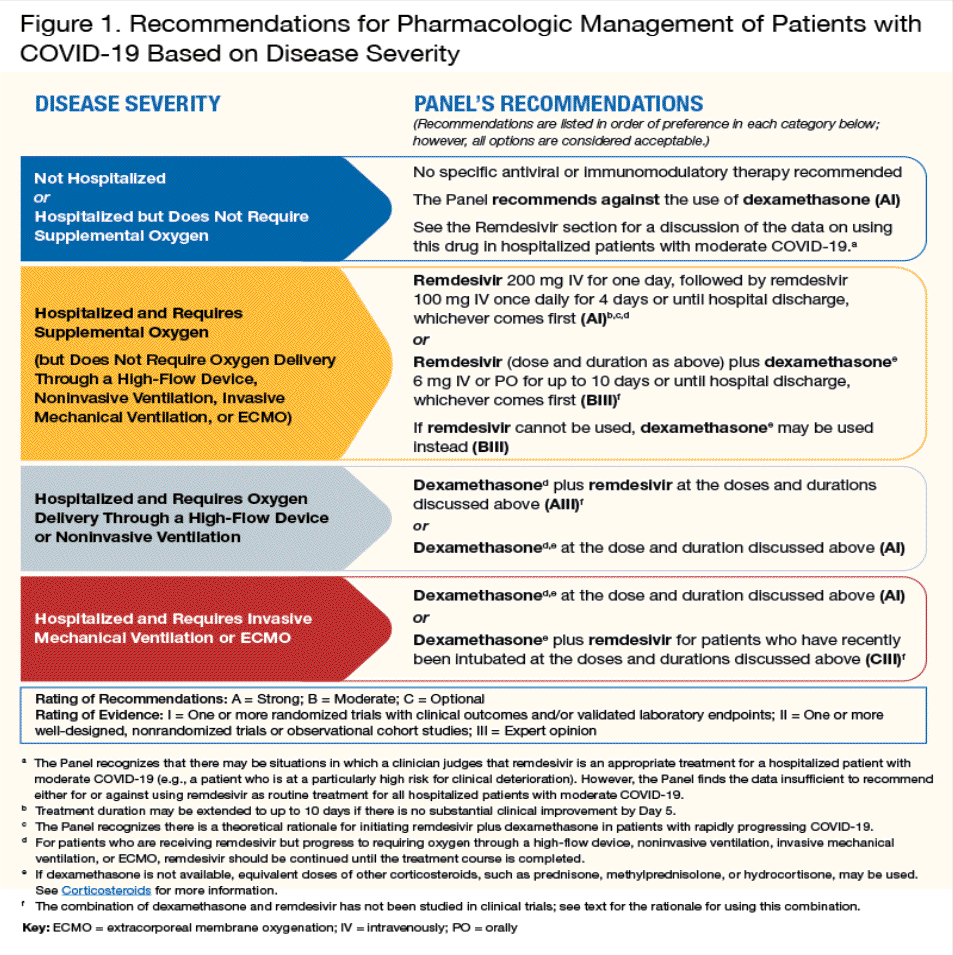
Objective
To characterize (1) the types of COVID-19 misinformation propagated by US physicians after vaccines became available, (2) the online platforms used, and (3) the characteristics of the physicians spreading misinformation.
They run the count from the beginning of the p
Landemic, but seem to want to erase the mass homicide that such false presumptions as theirs caused throughout 2020, by starting the discussion after the toxic, leaky non-"vaccines" became available (The CDC even had to
change the definition of vaccine to refer to these novel, deadly, gene therapies as vaccines, since they do not prevent infection or transmission of COVID).
America's Frontline Doctors that they demonize, would have been able to save millions of people worldwide if
Pharma's propagandist censors at YouTube/Google hadn't erased their video that had received 17 million views in the first 10 hours before it was erased. There never would have been cancellation of school, lockdowns or any of the other measures that caused so much destruction - particularly to our kids - with $20 early treatments:
America's Front Line Doctors Summit.com - page of summit videosDesign, Setting, and Participants Using US Centers for Disease Control and Prevention guidelines for the prevention and treatment of COVID-19 infection during the study window to define misinformation.....
Using Big Pharma's captured CDC is no way to "define misinformation" since they are some of the guiltiest propagators of it.
So
why didn't the authors of this BS inquire of the actual treating physicians that they demonized, as to what they were using that resulted in such great success in early treatment?
https://www.covid-19forum.org/index.php?board=3.0Because their interest was never in ferreting out the truth, but in propagating more propaganda for Big Pharma, through defamation of world class medical professionals with lies and deceit.
....structured searches of high-use social media platforms (Twitter, Facebook, Instagram, Parler, and YouTube) and news sources (The New York Times, National Public Radio) were conducted to identify COVID-19 misinformation communicated by US-based physicians between January 2021 and December 2022. Physicians’ state of licensure and medical specialty were identified. The number of followers for each physician on 4 major platforms was extracted to estimate reach and qualitative content analysis of the messages was performed.
Did they interview a single doctor that they demonize as spreading misinformation? No, because they knew in advance it would confirm those
front line treating physicians were propagating truth, not misinformation like the propagandist liars that created this evil hit piece.
Main Outcomes and Measures
Outcome measures included categories of COVID-19 misinformation propagated, the number and traits of physicians engaged in misinformation propagation, and the type of online media channels used to propagate misinformation and potential reach.
Results
The propagation of COVID-19 misinformation was attributed to 52 physicians in 28 different specialties across all regions of the country. General misinformation categories included vaccines,.....
I challenge these clowns and every other moron that advocates for volunteering to be lab rats in the trial of a
questionable corporation -
investigational, experimental,
genetically engineered,
chemically enhanced,
innate immune response reprogramming,
leaky,
escape mutant training,
gene therapy - the longer term consequences of which only God can know - to justify the risk in light of 99+% effective early treatment. They can't because it's impossible. Let alone a risk vs benefit analysis on top of that:
Vaccine RISK VS BENEFIT - Pragmatism (absurdly, put "hesitant") VS blind obedienceThere's not a single person on God's green earth that will even begin to know about the clot shot's safety, until a dozen or so years have passed
as even their demigod Fauci pointed out. But
with DNA perhaps being messed with, it will more likely be generations into the future, before anyone can know.
And that's not even taking into account the fact that
ALL prior efforts at mRNA vaccines for corona viruses in humans FAILED during the animal testing phase due to pathogenic priming - vaccine enhanced disease.
What is "vaccine-enhanced disease" or "pathogenic priming"?So before taking such an unknown risk, the following is the obvious question that needs to be answered before discussion about - what have become increasingly revealed as dangerous - clot shots begins.
Was a vaccine for COVID ever necessary, considering 99+% effective $20 early treatment remedies? medication, masks, and other (ie, conspiracy theories). Forty-two physicians (80.8%) posted vaccine misinformation, 40 (76.9%) propagated information in more than 1 category, and 20 (38.5%) posted misinformation on 5 or more platforms. Major themes identified included (1) disputing vaccine safety and effectiveness,
A whole forum section is dedicated to the alleged "safety and effectiveness" of the toxic clot shots.
https://www.covid-19forum.org/index.php?board=6.0There's the
42.8% greater all-cause mortality in Pfizer's vaccine group than placebo groupAs would seem to be demonstrated by the
Fifth-largest U.S. life insurer reporting a 163% rise in 2021 group (working age people) death-benefits paid, over 2020.
If so safe, why the
1,291 different "adverse events of special interest" in their trials, that
their propaganda ministry, the FDA, tried to hide over the next 50 years?
(2) promoting medical treatments lacking scientific evidence.....
Here they prove their abject ignorance as to even understanding what science is, since specific scientific evidence abounds, through the art and science of successful evidence-based COVID-19 treatment.
THE applied SCIENCE of COVID-19 treatmentPeer Reviewed Outpatient Study Finds hydroxycholorquine+Zn+Az Survival Rate 99%https://c19hcq.org/ "556 HCQ COVID-19 studies, 432 peer reviewed, 412 comparing treatment and control groups."
Hydroxychloroquine shown to reduce risk by
65% in early treatment, even though probably not one out of every 50 of those studies include ZINC, which all front line doctors know is the single most important element, of every early treatment protocol for COVID, in conjunction with a zinc ionophore.
.....and/or US Food and Drug Administration approval, (3) disputing mask-wearing effectiveness,
Again proving their abject ignorance. Like all interventions it's about the harm VS benefit.
More than 170 Comparative Studies and Articles on Mask Ineffectiveness and HarmsPossible toxicity of chronic carbon dioxide exposure associated with face mask..Several more articles on masks in this forum section:
https://www.covid-19forum.org/index.php?board=10.0 and (4) other (unsubstantiated claims, eg, virus origin, government lies, and other conspiracy theories).
Again, the FDA proves over and over how they work for their overlord Big Pharma rather than the American people. Even referring to ivermectin as "horse paste" when 4 billion doses have been administered to humans over 40 years. Do they refer to aspirin as "horse paste", since it's another therapeutic that is administered to horses in paste form?
Big Pharma's propaganda ministry, the FDA, horses around with IVM as COVID cureMeanwhile in Uttar Pradesh India through an early test and treat campaign, with
230 million people, 310,783 cases April, cut 97.1% in June, just 22 cases August thanks to ivermectin, zinc and the rest of their protocol.
Conclusions and Relevance
This fraudulent, homicidal, drivel has no relevance other than to try to further censor and intimidate world class successful front line treating physicians, that have saved millions of lives since the beginning of the pLandemic. These authors need to be held to account as all the other forces of evil that have been responsible for the mass homicide of a million Americans and millions more worldwide.
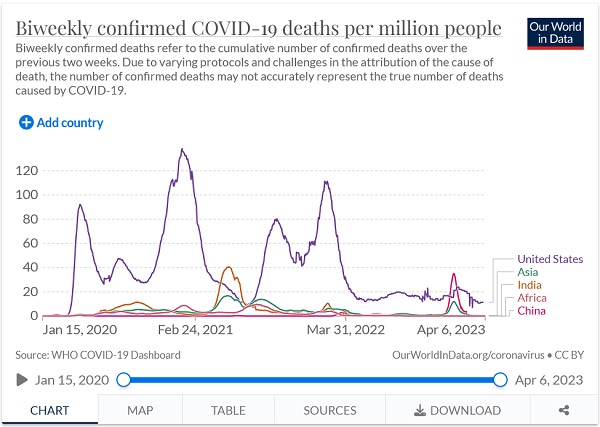
Homicidal nitwits that pretend lies are truth and that matters of irrefutable fact are false and perhaps worse of all that Big Pharma's captured government agencies were/are working in the interests of the American people rather than their overlords in Big Pharma. The following chart illustrates the fruit of liars such as those that constructed the brand of evil in their BS paper, as well as those that published it. Over a million Americans and millions more worldwide, were sacrificed on the alter of Big Pharma/government/media/journal/academia profit:
In this mixed-methods study of US physician propagation of COVID-19 misinformation on social media, results suggest widespread, inaccurate, and potentially harmful assertions made by physicians across the country who represented a range of subspecialties. Further research is needed to assess the extent of the potential harms associated with physician propagation of misinformation, the motivations for these behaviors, and potential legal and professional recourse to improve accountability for misinformation propagation.
Introduction
As of May 11, 2023, an estimated 1 128 000 COVID-19 deaths had occurred in the US,1 and nearly 14% of people infected by the COVID-19 virus have experienced the post–COVID-19 condition.2,3 As of December 2022, estimated death rates for unvaccinated persons in the US were 271 per 100 000 compared with 82 per 100 000 for those fully vaccinated, yet only 69.2% of eligible people had received the full primary vaccine series, and 15.5% had received the bivalent booster.1 Vaccination rates have varied by region throughout the pandemic despite widespread availability, with southeastern states having lower full primary series rates (52%) compared with northeastern states (80%).1 Other preventive behaviors, such as mask wearing and social distancing, have varied similarly by geographic region.4,5
Individual health behaviors related to COVID-19 have been attributed to complex social phenomena, including inconsistent recommendations by government entities early in the pandemic, mistrust of the scientific community, political polarization, and unclear or incorrect guidance from other sources.6-8 COVID-19 misinformation, defined as false, inaccurate, or misleading information according to the best evidence available at the time, and disinformation, defined as having an intentionally malicious purpose, have been ubiquitous on social media, despite major platforms’ COVID-19 misinformation policies.9 Medical misinformation was propagated long before the COVID-19 pandemic,10 but the internet increases reach and speed of dissemination, potentially exacerbating misinformation consequences during an unparalleled public health threat that has killed more than 7 million people across the globe.11-13
COVID-19 misinformation has been spread by many people on social medial platforms,14 but misinformation spread by physicians may be particularly pernicious.15 Physicians are often considered credible sources of medical and public health information, increasing the potential negative impact of physician-initiated misinformation. The US Food and Drug Administration (FDA) and others have called for action to limit the potential harm of physician-propagated COVID-19 misinformation.15,16 Despite the rising concerns voiced in news articles and opinion pieces, physician-propagated COVID-19 misinformation and its associated outcomes remain understudied.
This study aimed to address this gap in knowledge by examining COVID-19 misinformation communicated on social media platforms and other online sources by US physicians after vaccines were made available. Understanding the extent of this phenomenon, its potential impact, and associated professional, ethical, and legal ramifications may help to better understand the role that physician-propagated COVID-19 misinformation may have played in preventable COVID-19 deaths and mistrust in institutions.
Methods
Overview
This mixed-methods study sought to characterize the (1) type of COVID-19 misinformation physicians communicated online between January 1, 2021, and May 1, 2022; (2) social media and other online platforms where misinformation appeared; and (3) characteristics of the physicians. Physician age, sex, and race and ethnicity were not available on social media or other online postings. A decision was made to not infer these data from pictures or other means to avoid potential bias and misclassification. We defined COVID-19 misinformation as assertions unsupported by or contradicting US Centers for Disease Control and Prevention (CDC) guidance on COVID-19 prevention and treatment during the period assessed or contradicting the existing state of scientific evidence for any topics not covered by the CDC (eTable in Supplement 1). We conservatively classified inaccurate information as misinformation rather than disinformation because the intent of the propagator cannot be objectively assessed. The University of Massachusetts Institutional Review Board determined that this study did not meet criteria for human participant research. This study followed the Standards for Reporting Qualitative Research (SRQR) reporting guidelines.
Data Collection
First, we conducted structured searches of social media platforms and general web searches in late spring of 2022 to identify media containing COVID-19 misinformation attributed to US-based physicians, defined as using doctor of medicine (MD) or doctor of osteopathic medicine (DO) after their name and being licensed to practice medicine in the US at some time or never licensed but working in the US. The start date was selected in relation to the availability of the COVID-19 vaccines. Search terms included the following: “COVID,” “vaccine,” “doctor” or “physician,” “ineffective,” “pharmaceutical,” “medication,” “ivermectin,” “hydroxychloroquine,” and “purchase.” Search terms were refined based on initial searches to include “COVID misinformation,” “doctor” or “physician,” and/or “conspiracy theory.” Conspiracy theories were defined as communicating skepticism of all information that does not fit the theory, overinterpreting evidence that fits the theory, and/or evidence of internal inconsistency.17 The platforms searched were selected based on the volume of news articles, popularity, and searchability (Instagram, Twitter, YouTube, Facebook, Parler, TikTok, The New York Times, National Public Radio)18; if the findings on one platform indicated that another platform could have additional new data, it was added to the search list. Due to the large volume and repetitiveness of Tweets, Twitter searches focused initially on America’s Frontline Doctors’ Twitter profile because of the volume of COVID-19 misinformation in its Tweets,19 its large following, and the potential for physicians propagating misinformation to follow the page. Followers of the America’s Frontline Doctors’ page with an MD or DO in their header were traced on Twitter and other platforms as well. General internet searches using Google’s search engine were conducted to identify misinformation attributed to physicians in third party platforms, such as local news articles.
The following information was collected from each source: physician’s name, medical specialty, the state(s) in which they were currently or had been licensed, whether their license to practice was active, had lapsed, or been revoked based on state medical board site searches, when the misinformation was posted (if available), from what source it was found, and the number of followers the physician had (if the source was a social media platform). Misinformation was classified into the following categories: medication, vaccine, mask/distancing, and other unsubstantiated or false claims. After the initial searches were completed, the physicians’ names were searched on the social media platforms and through general online searches to identify misinformation they posted that may have been missed in the initial searches.
Statistical Analysis
Quantitative
Descriptive statistics were used to quantify the types of misinformation, the frequency in which they appeared, the platforms on which they were found, and characteristics of the physicians identified (eg, specialty and state(s) in which the physician was licensed). We calculated the total, median, and IQR for the number of followers on platforms with the highest volume of users (Twitter, Facebook, YouTube, Instagram) using Stata software, version 17 (StataCorp).
Qualitative
We performed directed qualitative content analysis20 of the misinformation using a validated rapid qualitative analysis approach.21 The analytic team (S.S. and M.D.) populated a templated summary table with misinformation text extracted from each media platform. The team divided the physician list and generated a summary of the misinformation associated with each of the physicians. In the second step of this analytic process, each team member individually identified pertinent and common themes, subthemes, and supporting quotes for each. After this was done individually, the team met to discuss their findings and combine the findings into a final list of themes and subthemes. Considerations regarding reflexivity included that S.G. is a public health professor and physician, and M.D. and S.S. are aspiring physicians, which may have increased sensitivity to potential harms.
Results
A total of 52 US physicians were identified as having communicated COVID-19 misinformation in the period assessed. All but 2 were or had been licensed to practice medicine in the US; the others were researchers. The 50 physicians who currently were or had been licensed represented 28 distinct medical specialties (3 of 50 had 2 different specialties; primary care was the most common overall [18 (36.0%)]) and they were licensed or working in 29 states across the US (Figure and Table 1). Forty-four of the 50 physicians (88.0%) held an active license in at least 1 state; 3 (6.0%) did not have an active license, 4 (8.0%) had had a license suspended or revoked, and 1 (2.0%) had active licenses in 2 states and revoked/suspended licenses in 2 other states. Nearly one-third (16 of 52) were affiliated with groups with a history of propagating medical misinformation, such as America’s Frontline Doctors. Specific types of misinformation included the following: (1) vaccines were unsafe and/or ineffective, (2) masks and/or social distancing did not decrease risk for contracting COVID-19, (3) medications for prevention or treatment were effective despite not having completed clinical trials or having been FDA approved, and (4) other (eg, conspiracy theories).
Quantitative Analyses
Most of the 52 physicians (40 [76.9%]) who posted misinformation did so in more than 1 of the 4 categories identified. Vaccine misinformation was posted by the majority (42 [80.8%]), followed by other misinformation (28 [53.8%]; eg, government and public health officials deliberately falsified COVID-19 statistics) and medication misinformation (27 [51.9%]).
Of these 52 physicians, 20 (38.5%) posted COVID-19 misinformation on 5 or more different social media platforms and 40 (76.9%) appeared on 5 or more third-party online platforms such as news outlets. Twitter was the most used platform, with 37 of the 52 physicians (71.2%) posting misinformation and a median of 67 400 followers (IQR, 12 900-204 000). Additional details of physicians’ reach by platforms and followers are in Table 2 and Table 3.
Qualitative Analyses
Major themes identified included the following: (1) claiming vaccines were unsafe and/or ineffective, (2) promoting unapproved medications for prevention or treatment, (3) disputing mask-wearing effectiveness, and (4) other misinformation, including unsubstantiated claims, eg, virus origin, government lies, and other conspiracy theories. Supportive quotes are listed in Table 4.
Claiming Vaccines Were Unsafe and/or Ineffective
The most common theme identified was physicians discouraging the public from receiving COVID-19 vaccines. Promoting fear and distrust of the vaccine and reliance on “natural” immunity were common subthemes.
Vaccine Ineffectiveness
Some of the misinformation propagated by physicians claimed that COVID-19 vaccines were ineffective at preventing COVID-19 spread. A common approach included circulating counts of positive case rates by vaccination status, claiming that most positive cases were among vaccinated individuals. This claim is technically true but misleading, as many more people are vaccinated, and the proportion of unvaccinated people who are infected is much higher.22 Some stated that the significant increase in case rates after the initial vaccine rollout was evidence for ineffectiveness.
Vaccine Risks
Assertions that COVID-19 vaccines were harmful was not supported by scientific evidence at the time. Unfounded claims included that the vaccines caused infertility, irreparable damage to one’s immune system, increased risk of developing a chronic illness for children, and a higher risk of cancer and death. Claims that myocarditis was common in children who received the vaccine and that the risks of myocarditis outweighed the risk of vaccination were also unfounded.23 Several physicians redistributed news articles with stories of individuals suddenly or mysteriously dying from the vaccine, despite evidence from the CDC confirming that deaths caused by a COVID vaccine were extremely rare (9 deaths for over 600 million doses administered in the US as of January 2023) and could be attributed only to the Johnson and Johnson COVID-19 vaccine, which was used much less frequently than other manufacturers’ vaccines in many countries.24
Promoting Unapproved Medications for Prevention or Treatment
Many of the identified physicians promoted the use of treatments that had not been tested or FDA approved for use in relation to COVID-19. The 2 most prominent medications promoted were ivermectin and hydroxychloroquine, which have been found to not be effective at treating COVID-19 infections in randomized clinical trials.25,26
What ignorant nitwits! 30 to 40% of medications are prescribed off-label for uses that they are not tested or approved by FDA for. And IVM and HCQ are two of the safest drugs on the planet as proven over the last 40 and 65 years.
Anecdotal Evidence of Effectiveness
Anecdotal personal experiences of successfully treating patients with untested medications were commonly used to support claims about safety and effectiveness, such as patients’ conditions were not improving before receiving the untested medication, but the patient recovered after starting the treatment.
Right. 3-1/2 years of "anecdotal" near 100% success, as demonstrated through millions of patients by front line treating physicians around the world, through the art and science of evidence-based COVID-19 treatment.
Dr. Zelenko recommendations of 3-23-2020 - 500 patients 0 deaths 0 hospitalizedDr Brian Tyson 20,000 COVID patients with 0 deaths in those treated before day 7MyFreeDoctor.com has treated 150,000 COVID patients with a 99.99% success rate230 million people, 310,783 cases April, cut 97.1% in June, just 22 cases AugustJAMA may be embarrassed into retracting this crap, but I will pledge to continue to rub their noses in it, and support any defamation suits that come their or the author's way.
Inaccurate Claims of Research-Based Evidence of Effectiveness
Many physicians posted links or screenshots to articles claiming that ivermectin decreased mortality and hospitalization and increased time to recovery and viral clearance. Although some of the articles appeared to be peer-reviewed, none were in high-quality peer-reviewed biomedical journals, and the FDA had not approved the use of these medications for treating COVID-19. At least 1 of the cited articles has been retracted due to misinterpretation of the data.27
Disputing Mask-Wearing Effectiveness
Many of the physicians propagating misinformation about masking effectiveness portrayed masks in a negative light. Claims centered on ineffectiveness, harm, or both.
Ineffectiveness
Most of the misinformation propagated about wearing protective masks asserted that studies conducted before the pandemic definitively concluded that masks do not prevent the spread of respiratory viral infections. Additionally, data showing rising cases in areas enforcing mask mandates were interpreted to mean that the mandates did nothing to slow the spread of infection.
Negative Consequences
Allegations of consequences of mask wearing included medical and social or developmental effects, all of which were unfounded.28 Alleged medical consequences included claims that wearing a face mask restricts one’s oxygen, increases the amount of carbon dioxide being inhaled, and causes mask wearers to inhale bacteria that gets trapped. Many physicians focused on negative consequences related to children and mask mandates in schools, claiming that masks interfered with social development despite lack of evidence and that requiring children to wear masks was a form of child abuse.
Other Misinformation
This misinformation category included conspiracy theories related to domestic and foreign governments and pharmaceutical companies. Theories related to the government included the following: (1) the COVID-19 pandemic was planned by government officials—the “plandemic”; (2) government and public health officials withheld key information regarding COVID-19 from the public, such as hydroxychloroquine effectiveness, falsified statistics to make the virus appear more severe, and censored information that challenged government messaging; (3) the virus originated in a laboratory in China, which contradicted scientific evidence at the time; and (4) the virus was part of a National Institutes of Health–funded study, was leaked, and that the leak was covered up by government and public health officials. Theories related to pharmaceutical companies included that they played a role in discouraging the use of ivermectin and hydroxychloroquine because these medications were inexpensive and easily accessible, and pharmaceutical companies benefited from the promotion of more novel and expensive treatments.
Discussion
This study was the first, to our knowledge, to identify the types of COVID-19 misinformation propagated by US physicians on social media and the platforms they used, as well as characterize the physicians who spread the misinformation. The content of misinformation physicians spread was similar to the misinformation spread by others; this study contributes new information about the range of specialties and regions of the country the physicians represented. The widely varying number of followers on social media for each physician suggested that the impact of any individual physician’s social media postings also may vary.
Some of the physicians identified belonged to organizations that have been propagating medical misinformation for decades,10 but these organizations became more vocal and visible in the context of the pandemic’s public health crisis, political divisiveness, and social isolation. Understanding the motivation for misinformation propagation is beyond the scope of this study, but it has become an increasingly profitable industry within and outside of medicine. For example, America’s Frontline Doctors implemented a telemedicine service that charged $90 per consult, primarily to prescribe hydroxychloroquine and ivermectin for COVID-19 to patients across the country, profiting at least $15 million from the endeavor.29 Twitter’s elimination of safeguards against misinformation30 and the absence of federal laws regulating medical misinformation on social media platforms suggest that misinformation about COVID-19 and other medical misinformation is likely to persist and may increase. Deregulation of COVID-19 misinformation on social media platforms may have far-reaching implications because consumers may struggle to evaluate the accuracy of the assertions made.31
National physicians’ organizations, such as the American Medical Association, have called for disciplinary action for physicians propagating COVID-19 misinformation,32 but stopping physicians from propagating COVID-19 misinformation outside of the patient encounter may be challenging.33 Although professional speech may be regulated by courts34 and the FDA has been called on to address medical misinformation,16 few physicians appear to have faced disciplinary action. Factors such as licensing boards’ lack of resources available to dedicate toward monitoring the internet35 and state government officials’ challenges to medical boards’ authority to discipline physicians propagating misinformation36 may limit action.
Scientific evidence depends on a body of accumulated research to inform practice and guidelines and the evidence depends on the best quality research available at any given time. A recent Cochrane Review has been misinterpreted to have definitively shown that wearing masks does not reduce transmission of respiratory viruses and has been used to support assertions that masks definitively “do not work.”37 Although the Federal Bureau of Investigation and Department of Energy presented a theory to Congress that the COVID-19 virus was the result of a laboratory leak,38 scientific evidence and a more recent report from the Office of the Director of National Intelligence demonstrate lack of evidence for a laboratory leak and favor a zoonotic origin of the virus.39,40 These recent challenges to prior understandings illuminate the importance of transparency and reproducibility of the process by which conclusions are drawn.
Limitations
This study had some limitations. We conducted the study in the spring of 2022, after many major social media platforms had begun to establish policies to combat the propagation of COVID-19 misinformation, which means that the current study may underrepresent the extent of misinformation present before these policies were put in place. On some platforms (eg, Twitter), we were unable to analyze all posts by individuals due to the high volume of Tweets and degree of repetition. This study focused on online platforms whose content was readily accessible to the public; different approaches to identifying misinformation and searches of less used platforms might identify other physicians and include other topics. Misinformation disseminated in other ways, such as during clinical care, was not captured. Vaccines had been approved at the start of the period studied, but accessibility may have varied in the early days of the initial rollout. Finally, the state of scientific evidence for COVID-19 guidelines has evolved rapidly over the course of the pandemic, and this study represents a cross-section of time. The current evidence base for preventive and treatment practices, such as duration of vaccine effectiveness, may differ from the evidence base during the study time frame.
Conclusions
Results of this mixed-methods study of the propagation of COVID-19 misinformation by US physicians on social media suggest that physician-propagated misinformation has reached many people during the pandemic and that physicians from a range of specialties and geographic regions have contributed to the “infodemic.” High-quality, ethical health care depends on inviolable trust between health care professionals, their patients, and society. Understanding the degree to which the misinformation about vaccines, medications, masks, and conspiracy theories spread by physicians on social media influences behaviors that put patients at risk for preventable harm, such as illness or death, will help to guide actions to regulate content or discipline physicians who participate in misinformation propagation related to COVID-19 or other conditions. A coordinated response by federal and state governments and the profession that takes free speech carefully into account is needed.
Back to top
Article Information
Accepted for Publication: July 6, 2023.
Published: August 15, 2023. doi:10.1001/jamanetworkopen.2023.28928
Open Access: This is an open access article distributed under the terms of the CC-BY License. © 2023 Sule S et al. JAMA Network Open.
Corresponding Author: Sarah L. Goff, MD, PhD, Department of Health Promotion and Policy, School of Public Health and Health Sciences, University of Massachusetts, 715 N Pleasant St, Amherst, MA 01002 (sgoff@umass.edu).
Author Contributions: Dr Goff had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Mss Sule and DaCosta are considered co–first authors.
Concept and design: Sule, Gilson, Goff.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Sule, DaCosta.
Statistical analysis: Sule, DaCosta, Gilson.
Administrative, technical, or material support: DaCosta, DeCou, Gilson, Goff.
Supervision: DaCosta, Goff.
Conflict of Interest Disclosures: Dr Wallace reported contributing to this work while she was a student at University of Massachusetts Amherst, before and outside of her official capacity as a government employee. No other disclosures were reported.
Funding/Support: The study was funded via internal support by the University of Massachusetts (Dr Goff).
Role of the Funder/Sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclaimer: The views expressed here are those of the authors and do not represent the official policy or position of the US Department of Veteran Affairs or the US government.
Data Sharing Statement: See Supplement 2.
References
1.
US Centers for Disease Control and Prevention. COVID data tracker. Centers for Disease Control and Prevention. Accessed May 18, 2023. https://covid.cdc.gov/covid-data-tracker
2.
Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B. Global prevalence of post–coronavirus disease 2019 (COVID-19) condition or long covid: a meta-analysis and systematic review. J Infect Dis. 2022;226(9):1593-1607. doi:10.1093/infdis/jiac136PubMedGoogle ScholarCrossref
3.
Perlis RH, Santillana M, Ognyanova K, et al. Prevalence and correlates of long COVID symptoms among US adults. JAMA Netw Open. 2022;5(10):e2238804. doi:10.1001/jamanetworkopen.2022.38804
ArticlePubMedGoogle ScholarCrossref
4.
Katz J, Sanger-Katz M, Quealy K. A detailed map of who is wearing masks in the US. Accessed May 19, 2023. https://www.nytimes.com/interactive/2020/07/17/upshot/coronavirus-face-mask-map.html
5.
Kemmelmeier M, Jami WA. mask wearing as cultural behavior: an investigation across 45 US states during the COVID-19 pandemic. Front Psychol. 2021;12:648692. doi:10.3389/fpsyg.2021.648692PubMedGoogle ScholarCrossref
6.
Kerr J, Panagopoulos C, van der Linden S. Political polarization on COVID-19 pandemic response in the US. Pers Individ Dif. 2021;179:110892. doi:10.1016/j.paid.2021.110892PubMedGoogle ScholarCrossref
7.
Evanega S, Lynas M, Adams J, Smolenyak K. Quantifying sources and themes in the COVID-19 “infodemic.” Accessed May 16, 2023. https://allianceforscience.org/wp-content/uploads/2020/09/Evanega-et-al-Coronavirus-misinformationFINAL.pdf
8.
Gollwitzer A, Martel C, Brady WJ, et al. Partisan differences in physical distancing are linked to health outcomes during the COVID-19 pandemic. Nat Hum Behav. 2020;4(11):1186-1197. doi:10.1038/s41562-020-00977-7PubMedGoogle ScholarCrossref
9.
Tan C. Regulating disinformation on Twitter and Facebook. Griffith Law Rev. 2022;31(4):513-536. doi:10.1080/10383441.2022.2138140Google ScholarCrossref
10.
Association of American Physicians and Surgeons. Home page. Accessed May 19, 2023. https://aapsonline.org/
11.
Muhammed T S, Mathew SK. The disaster of misinformation: a review of research in social media. Int J Data Sci Anal. 2022;13(4):271-285. doi:10.1007/s41060-022-00311-6PubMedGoogle ScholarCrossref
12.
Rosenberg H, Syed S, Rezaie S. The Twitter pandemic: the critical role of Twitter in the dissemination of medical information and misinformation during the COVID-19 pandemic. CJEM. 2020;22(4):418-421. doi:10.1017/cem.2020.361PubMedGoogle ScholarCrossref
13.
Tsao SF, Chen H, Tisseverasinghe T, Yang Y, Li L, Butt ZA. What social media told us in the time of COVID-19: a scoping review. Lancet Digit Health. 2021;3(3):e175-e194. doi:10.1016/S2589-7500(20)30315-0PubMedGoogle ScholarCrossref
14.
ABC News. Who is spreading COVID-19 misinformation and why. Accessed May 20, 2023. https://abcnews.go.com/US/spreading-covid-19-misinformation/story?id=70615995
15.
Rubin R. When physicians spread unscientific information about COVID-19. JAMA. 2022;327(10):904-906. doi:10.1001/jama.2022.1083
ArticlePubMedGoogle ScholarCrossref
16.
Kadakia KT, Beckman AL, Krumholz HM. A prescription for the US FDA for the regulation of health misinformation. Nat Med. 2023;29(3):525-527. doi:10.1038/s41591-022-02172-9PubMedGoogle ScholarCrossref
17.
Lewandowsky S, Cook J. The conspiracy theory handbook. Accessed May 16, 2023. https://www.climatechangecommunication.org/wp-content/uploads/2020/03/ConspiracyTheoryHandbook.pdf
18.
Search Engine Journal. The top 10 social media sites & platforms. Accessed May 20, 2023. https://www.searchenginejournal.com/social-media/biggest-social-media-sites/
19.
Kouzy R, Abi Jaoude J, Kraitem A, et al. Coronavirus goes viral: quantifying the COVID-19 misinformation epidemic on Twitter. Cureus. 2020;12(3):e7255. doi:10.7759/cureus.7255PubMedGoogle ScholarCrossref
20.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277-1288. doi:10.1177/1049732305276687PubMedGoogle ScholarCrossref
21.
Gale RC, Wu J, Erhardt T, et al. Comparison of rapid vs in-depth qualitative analytic methods from a process evaluation of academic detailing in the Veterans Health Administration. Implement Sci. 2019;14(1):11. doi:10.1186/s13012-019-0853-yPubMedGoogle ScholarCrossref
22.
Egger S, Egger G. The vaccinated proportion of people with COVID-19 needs context. Lancet. 2022;399(10325):627. doi:10.1016/S0140-6736(21)02837-3PubMedGoogle ScholarCrossref
23.
Diaz GA, Parsons GT, Gering SK, Meier AR, Hutchinson IV, Robicsek A. Myocarditis and pericarditis after vaccination for COVID-19. JAMA. 2021;326(12):1210-1212. doi:10.1001/jama.2021.13443
ArticlePubMedGoogle ScholarCrossref
24.
US Centers for Disease Control and Prevention. Selected adverse events reported after COVID-19 vaccination. Accessed May 20, 2023. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html
25.
Self WH, Semler MW, Leither LM, et al; National Heart, Lung, and Blood Institute PETAL Clinical Trials Network. Effect of hydroxychloroquine on clinical status at 14 days in hospitalized patients with COVID-19: a randomized clinical trial. JAMA. 2020;324(21):2165-2176. doi:10.1001/jama.2020.22240
ArticlePubMedGoogle ScholarCrossref
26.
Roman YM, Burela PA, Pasupuleti V, Piscoya A, Vidal JE, Hernandez AV. Ivermectin for the treatment of coronavirus disease 2019: a systematic review and meta-analysis of randomized controlled trials. Clin Infect Dis. 2022;74(6):1022-1029. doi:10.1093/cid/ciab591PubMedGoogle ScholarCrossref
27.
Efimenko I, Nackeeran S, Jabori S, Zamora JAG, Danker S, Singh D. Removed: treatment with ivermectin is associated with decreased mortality in COVID-19 patients: analysis of a national federated database. Int J Infect Dis. 2022;116S:S40. doi:10.1016/j.ijid.2021.12.096PubMedGoogle ScholarCrossref
28.
US Centers for Disease Control and Prevention. Science brief: community use of masks to control the spread of SARS-CoV-2. Accessed July 3, 2023. https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html
29.
TIME. How “America’s frontline doctors” sold access to bogus COVID-19 treatments—and left patients in the lurch. Accessed May 20, 2023. https://time.com/6092368/americas-frontline-doctors-covid-19-misinformation/
30.
AP News. Twitter ends enforcement of COVID misinformation policy. Accessed May 20, 2023. https://apnews.com/article/twitter-ends-covid-misinformation-policy-cc232c9ce0f193c505bbc63bf57ecad6
31.
Pennycook G, McPhetres J, Zhang Y, Lu JG, Rand DG. Fighting COVID-19 misinformation on social media: experimental evidence for a scalable accuracy-nudge intervention. Psychol Sci. 2020;31(7):770-780. doi:10.1177/0956797620939054PubMedGoogle ScholarCrossref
32.
American Medical Association. AMA details plan to stop the public health “infodemic.” Accessed May 21, 2023. https://www.ama-assn.org/delivering-care/public-health/ama-details-plan-stop-public-health-infodemic
33.
Sage WM, Yang YT. Reducing “COVID-19 misinformation” while preserving free speech. JAMA. 2022;327(15):1443-1444. doi:10.1001/jama.2022.4231
ArticlePubMedGoogle ScholarCrossref
34.
Haupt CE. Professional speech. Accessed May 19, 2023. https://www.yalelawjournal.org/article/professional-speech
35.
Brumfiel G. This doctor spread false information about COVID—she still kept her medical license. Accessed May 21, 2023. https://www.npr.org/sections/health-shots/2021/09/14/1035915598/doctors-covid-misinformation-medical-license
36.
Farmer B. As state medical boards try to stamp out COVID misinformation, some in GOP push back. Accessed May 21, 2023. https://www.npr.org/sections/health-shots/2022/02/14/1077689734/as-state-medical-boards-try-to-stamp-out-covid-misinformation-some-in-gop-push-b
37.
Cochrane.org. Statement on “physical interventions to interrupt or reduce the spread of respiratory viruses” review. Accessed May 21, 2023. https://www.cochrane.org/news/statement-physical-interventions-interrupt-or-reduce-spread-respiratory-viruses-review
38.
US House Committee on Oversight. COVID origins, part 2 hearing wrap up: intelligence community officials provide further evidence that COVID-19 originated in a Wuhan lab. Accessed May 21, 2023. https://oversight.house.gov/release/covid-origins-part-2-hearing-wrap-up-intelligence-community-officials-provide-further-evidence-that-covid-19-originated-in-a-wuhan-lab/
39.
Alwine JC, Casadevall A, Enquist LW, Goodrum FD, Imperiale MJ. A critical analysis of the evidence for the SARS-CoV-2 origin hypotheses. J Virol. 2023;97(4):e0036523. doi:10.1128/jvi.00365-23PubMedGoogle ScholarCrossref
40.
Office of the Director of National Intelligence. Potential links between the Wuhan Institute of Virology and the origin of the COVID-19 pandemic. Accessed July 3, 2023. https://www.dni.gov/files/ODNI/documents/assessments/Report-on-Potential-Links-Between-the-Wuhan-Institute-of-Virology-and-the-Origins-of-COVID-19-20230623.pdf
JAMA Network Open
Content
Home New Online Current Issue
Podcast
JAMA Network Open Editors' Summary
Journal Information
For Authors Editors & Publishers RSS Contact Us
JN Learning / CME Store Apps Jobs Institutions Reprints & Permissions
JAMA Network
Publications
JAMA JAMA Network Open JAMA Cardiology JAMA Dermatology JAMA Health Forum JAMA Internal Medicine JAMA Neurology JAMA Oncology JAMA Ophthalmology JAMA Otolaryngology–Head & Neck Surgery JAMA Pediatrics JAMA Psychiatry JAMA Surgery Archives of Neurology & Psychiatry (1919-1959)
Sites
Art and Images in Psychiatry Artificial Intelligence (AI) Resource Center Best of the JAMA Network Clinical Crosswords from JAMA Coronavirus Resource Center Evidence-Based Medicine: An Oral History Fishbein Fellowship Genomics and Precision Health Hypertension


